Successful application of dietary ketogenic metabolic therapy in patients with glioblastoma: a clinical study
生酮饮食代谢疗法在胶质母细胞瘤患者中的成功应用:一项临床研究
Andreas K iry t to poul os 1, Athanasios E. Evan geli ou 2*, Irene Katsanika?, loannis Bou kov in as 4, Nikolaos Foroglou5, Basilios Zountsas°, Angeliki Cheva', Vaios Niko lo poul os 8, Thomas Za rambo uk as 8, Tomas Duraj?, Thomas N. Seyfried? and Martha Spilioti1
Andreas K iry t to poul os 1, Athanasios E. Evan geli ou 2*, Irene Katsanika?, loannis Bou kov in as 4, Nikolaos Foroglou5, Basilios Zountsas°, Angeliki Cheva', Vaios Niko lo poul os 8, Thomas Za rambo uk as 8, Tomas Duraj?, Thomas N. Seyfried? and Martha Spilioti1
1 Department of Neurology, Aristotle University of Thessaloniki, Thessaloniki, Greece, 2 Division of Child Neurology, St Luke's Hospital, Thessaloniki, Greece, 3 Department of Diet and Nutrition, Papa georgi ou General Hospital, Thessaloniki, Greece, 4 Bioclinic Thessaloniki Medical Oncology Unit, Thessaloniki, Greece, 5 Department of Neurosurgery, Aristotle University of Thessaloniki, Thessaloniki, Greece, 6 Department of Neurosurgery, St Luke's Hospital, Thessaloniki, Greece, 7 Department of Pathology, Faculty of Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece, 9 Department of Biology, Boston College, Chestnut Hill, MA, United States
1 塞萨洛尼基亚里士多德大学神经内科,希腊塞萨洛尼基,2 圣卢克医院儿童神经科,希腊塞萨洛尼基,3 帕帕乔治乌总医院饮食营养科,希腊塞萨洛尼基,4 塞萨洛尼基生物诊所肿瘤内科,希腊塞萨洛尼基,5 塞萨洛尼基亚里士多德大学神经外科,希腊塞萨洛尼基,6 圣卢克医院神经外科,希腊塞萨洛尼基,7 塞萨洛尼基亚里士多德大学医学院病理科,希腊塞萨洛尼基,9 波士顿学院生物系,美国马萨诸塞州栗树山
Introduction: Glioblastoma multiforme (GBM) ranks as one of the most aggressive primary malignant tumor affecting the brain. The persistent challenge of treatment failure and high relapse rates in GBM highlights the need for new treatment approaches. Recent research has pivoted toward exploring alternative therapeutic methods, such as the ketogenic diet, for GBM.
引言:多形性胶质母细胞瘤 (GBM) 是最具侵袭性的原发性恶性脑肿瘤之一。GBM治疗失败和高复发率的持续挑战凸显了对新治疗方法的迫切需求。近期研究开始转向探索替代疗法,例如生酮饮食在GBM中的应用。
Methods: A total of 18 patients with GBM, 8 women and 10 men, aged between 34 and 75 years participated in a prospective study, examining the impact of ketogenic diet on tumor progression. The pool of patients originated from our hospital during the period from January 2016 until July 2021 and were followed until January 2024. As an assessment criterion, we set an optimistic target for adherence to the ketogenic diet beyond 6 months. We considered the therapeutic combination successful if the survival reached at least 3 years.
方法:共有18名胶质母细胞瘤(GBM)患者(8名女性和10名男性,年龄在34至75岁之间)参与了一项前瞻性研究,旨在检验生酮饮食对肿瘤进展的影响。这些患者于2016年1月至2021年7月期间来自我院,并随访至2024年1月。我们将坚持生酮饮食超过6个月设定为乐观的评估标准。若患者生存期达到至少3年,则视为治疗组合成功。
Results: Among the 18 patients participating in the study, 6 adhered to the ketogenic diet for more than 6 months. Of these patients, one patient passed away 43 months after diagnosis, achieving a survival of 3 years; another passed away at 36 months, narrowly missing the 3-year survival mark; and one is still alive at 33 months post-diagnosis but has yet to reach the 3-year milestone and is, therefore, not included in the final survival rate calculation. The remaining 3 are also still alive, completing 84,43 and 44 months of life, respectively. Consequently, the survival rate among these patients is 4 out of 6, or $66.7%$ . Of the 12 patients who did not adhere to the diet, only one reached 36 months of survival, while the rest have died in an average time of $15.7\pm6.7$ months, with a 3-year survival rate of $8.3%$ . Comparing the survival rates of the two groups, we see that the difference is $58.3%$ ( $66.7%$ versus $8.3%$ ) and is statistically significant with $p<0.05$ (0.0114) and $X^{2}=6.409\$ .
结果:在参与研究的18名患者中,有6人坚持生酮饮食超过6个月。其中1例患者在确诊43个月后去世,实现3年生存期;另1例于36个月时离世,以微小差距未达3年生存标记;还有1例确诊后存活33个月,因尚未达到3年里程碑而未计入最终生存率统计。其余3例目前仍存活,分别完成84、43和44个月生存期。因此,该组患者生存率为4/6(66.7%)。未坚持饮食的12名患者中,仅1例达到36个月生存期,其余患者平均在(15.7±6.7)个月内死亡,3年生存率为8.3%。两组生存率比较显示差异达58.3%(66.7% vs 8.3%),具有统计学显著性(p<0.05)(0.0114),X²=6.409\$。
Discussion: The outcomes observed in these patients offer promising insights into the potential benefits of the ketogenic diet on the progression of glioblastoma multiforme when compared to those who did not follow the diet consistently.
讨论:与未坚持生酮饮食的患者相比,这些患者观察到的结果为生酮饮食对多形性胶质母细胞瘤进展的潜在益处提供了有希望的见解。
KEYWORDS ketogenic, glioblastoma, diet, multiforme, metabolic, brain, tumor
关键词 生酮饮食、胶质母细胞瘤、饮食、多形性、代谢、脑部、肿瘤
1 Introduction
1 引言
Glioblastoma (GBM) is the most common primary malignant tumor of the brain and central nervous system. It accounts for $14.5%$ of all central nervous system tumors and $48.6%$ of malignant central nervous system tumors (1). Despite surgical excision (total or subtotal), followed by adjuvant radiotherapy and chemotherapy with temozolomide, patients with newly diagnosed GBM have a median overall survival of 12–18 months, with $<10%$ surviving beyond 5 years (2, 3). Additionally, GBM is an invasive tumor and usually recurs within 32–36 weeks of initial diagnosis, despite maximal treatment.
胶质母细胞瘤 (GBM) 是大脑和中枢神经系统最常见的原发性恶性肿瘤。它占所有中枢神经系统肿瘤的 $14.5%$ 和恶性中枢神经系统肿瘤的 $48.6%$ (1)。即使经过手术切除 (全切或次全切) 并辅以放疗和替莫唑胺化疗,新诊断的 GBM 患者中位总生存期仅为 12-18 个月,$<10%$ 的患者能存活超过 5 年 (2, 3)。此外,GBM 具有侵袭性,即使在接受最大程度治疗后,通常也会在初次诊断后 32-36 周内复发。
The almost universal relapse and poor long-term prognosis highlight the need for new treatment approaches. Thus, in recent years, the research community has turned to the discovery of alternative therapeutic strategies for GBM, such as dietary ketogenic metabolic therapy (KMT). Dietary KMT is defined as a synergistic precision nutrition approach, incorporating biomarker-driven ketogenic diets, fasting and fasting-mimicking diets, as well as other lifestyle interventions (4, 5). Monitoring of adherence should be performed by quantitative, unbiased biomarkers, such as the glucose-ketone index (GKI) (6). In particular, recent advancements in our understanding of cancer metabolism have led to renewed interest in Warburg’s theory of carcinogen es is (7–9). According to this theory, malignant cells are characterized by distinct structural and functional mitochondrial abnormalities, leading to compensatory metabolic dependencies. The main metabolic phenotype of GBM is a high glycolytic rate with lactic acid fermentation due to loss of efficiency in the respiratory cycle, despite ample mutational heterogeneity and secondary metabolic reprogramming (10). Unlike normal brain cells, that have evolved to metabolize ketone bodies for energy when glucose availability is low, GBM cells depend on glycolysis for growth and are unable to efficiently metabolize ketones due to impaired mitochondrial function (11–13). This metabolic deficiency isolates cancer cells from normal cells from a metabolic perspective, regardless of their somatic mutation landscape.
普遍存在的复发和不良长期预后凸显了新治疗方法的必要性。因此,近年来研究界开始探索胶质母细胞瘤(GBM)的替代治疗策略,例如生酮代谢疗法(KMT)。膳食KMT被定义为一种协同精准营养方法,整合了生物标志物驱动的生酮饮食、禁食与模拟禁食饮食以及其他生活方式干预措施(4, 5)。治疗依从性应通过葡萄糖-酮体指数(GKI)等定量、无偏见的生物标志物进行监测(6)。特别是,近期癌症代谢研究进展重新引发了人们对Warburg致癌理论的关注(7-9)。该理论认为,恶性细胞的典型特征是线粒体存在独特的结构和功能异常,从而导致代偿性代谢依赖。尽管存在显著的突变异质性和继发性代谢重编程,GBM的主要代谢表型仍是因呼吸循环效率低下导致的高糖酵解速率伴乳酸发酵(10)。与能适应低葡萄糖环境而代谢酮体供能的正常脑细胞不同,GBM细胞依赖糖酵解生长,且由于线粒体功能受损无法有效代谢酮体(11-13)。这种代谢缺陷从代谢角度将癌细胞与正常细胞区分开来,不受体细胞突变背景影响。
Based on the above observations, interest is growing in designing metabolism-based treatments for cancer in general and primary brain tumors in particular. Specifically, GBM cells lack metabolic versatility due to mitochondrial abnormalities and are largely dependent on glucose and glutamine for energy and biosynthesis (7, 8). Moreover, Warburg discovered that the excessive amount of glucose consumed by tumor tissues is fermented to lactate despite the presence of oxygen, rather than oxidized via mitochondrial respiration (6). However, it is still unknown to what degree other pure ly oxidative fuels, such as lactate, fatty acids, or ketone bodies, could contribute to cell survival and/or proliferation under relative glycolytic depletion in vivo. It is hypothesized that cancer cells cannot compensate for the simultaneous inhibition of glycolysis and glut amino lysis via ketone body metabolism due to acquired metabolic inflexibility (14). This hypothesis is strengthened by the presence of triglyceride-rich cytoplasmic lipid droplets in many malignant cancers. Recent research work has provided strong evidence that the presence of cytoplasmic lipid droplets and the aerobic fermentation commonly seen in most malignant cancers can serve together as biomarkers for oxidative phosphor yl ation inefficiency (15).
基于上述观察,人们对于设计基于代谢的癌症治疗方案,尤其是针对原发性脑肿瘤的兴趣日益增长。具体而言,由于线粒体异常,GBM细胞缺乏代谢灵活性,主要依赖葡萄糖和谷氨酰胺获取能量并进行生物合成 (7, 8)。此外,Warburg发现,尽管存在氧气,肿瘤组织消耗的过量葡萄糖仍会发酵为乳酸,而非通过线粒体呼吸氧化 (6)。然而,在体内相对糖酵解耗竭的情况下,其他纯氧化燃料(如乳酸、脂肪酸或酮体)能在多大程度上促进细胞存活和/或增殖仍不清楚。据推测,由于获得性代谢不灵活性,癌细胞无法通过酮体代谢来补偿糖酵解和谷氨酰胺分解的同时抑制 (14)。许多恶性癌症中存在富含甘油三酯的胞质脂滴,进一步支持了这一假说。最近的研究工作提供了强有力的证据,表明胞质脂滴的存在以及在大多数恶性癌症中常见的有氧发酵,可以共同作为氧化磷酸化效率低下的生物标志物 (15)。
Thus, with the current failure of che mo radiotherapy to improve long-term outcomes in GBM, as well as the proposed inability of GBM cells to efficiently oxidize ketone bodies when glycolysis is sufficiently limited, dietary KMT has been tested in the clinic to weaken the tumor and protect healthy cells during cytotoxic treatments (16, 17). Glucose and ketone metabolism in normal and cancer cells is illustrated in Figures 1A,B, 2A,B. While there is adequate experimental evidence supporting the beneficial effects of KMT on brain tumors, clinical testing is still ongoing (13, 18, 19). Most of the translational research to date involved case series and pilot clinical trials (20–24). In experimental models, KMT reduces glycolytic flux in cancer cells and increases ketolysis in non-tumoral cells, while also enhancing tumorreactive immune responses (25). Therefore, biomarker-driven ketogenic diets could be a complementary therapeutic intervention for patients with GBM, aiming to slow tumor growth, potentiate standard cytotoxic therapies, and extend longterm survival.
因此,鉴于当前化疗放疗未能改善胶质母细胞瘤(GBM)的长期预后,以及提出的当糖酵解被充分限制时GBM细胞无法有效氧化酮体的观点,生酮代谢疗法(KMT)已在临床中进行测试,旨在细胞毒性治疗期间削弱肿瘤并保护健康细胞 (16, 17)。图1A,B和2A,B展示了正常细胞与癌细胞中的葡萄糖及酮体代谢情况。虽然现有充分实验证据支持生酮代谢疗法对脑肿瘤的积极作用,但相关临床试验仍在进行中 (13, 18, 19)。目前大多数转化研究涉及病例系列和初步临床试验 (20–24)。在实验模型中,生酮代谢疗法可降低癌细胞的糖酵解通量,同时增强非肿瘤细胞的酮体分解能力,并能提升肿瘤反应性免疫应答 (25)。因此,基于生物标志物的生酮饮食可能成为GBM患者的补充治疗手段,以期延缓肿瘤生长、增强标准细胞毒性疗法效果并延长长期生存期。
Based on Warburg’s theory and expanding upon the above mentioned experimental and clinical data, we offered ketogenic diet therapy to a cohort of 18 GBM patients. GBM was chosen as a target due to well-characterized metabolic dependency upon glycolysis and poor prognosis despite maximal standard therapies (3, 26, 27). Our decision to offer ketogenic diet therapy to our patients was strengthened by the fact that no significant side effects have been reported in previous safety and feasibility studies (28, 29).
基于Warburg的理论并结合上述实验与临床数据,我们对18名GBM患者实施了生酮饮食疗法。选择GBM作为研究对象,是因为该肿瘤具有明确的糖酵解代谢依赖性,且即使采用标准疗法预后仍较差 (3, 26, 27)。此前安全性和可行性研究中未报告显著副作用 (28, 29),这一事实增强了我们对患者实施生酮饮食疗法的信心。
2 Materials and methods
2 材料与方法
2.1 Study design
2.1 研究设计
A total of 18 patients with GBM, 8 women and 10 men, between 34 and 75 years of age (median age 57.5 years) participated in our prospective study evaluating the effects of ketogenic diet therapy on tumor progression. The pool of patients originated from our hospital and from a collaborating oncologist during the period from January 2016 until July 2021 and were followed until January 2024. The study was conducted in accordance with the1975 declaration of Helsinki and received prior approval from the ethics committee of our university (PN 1232/16). A double-blind design was planned, but due to the rapid progression of the disease, a survival of 3 years or more was considered as a success factor (30, 31). All subjects were referred to our hospital’s outpatient clinic for a general neurological assessment, including neurological status and MRI evaluation. A detailed laboratory evaluation was also performed, including the following: complete blood count, biochemical tests (electrolytes, blood glucose, trans a minas es, cholesterol, triglycerides, thyroid hormones), electrocardiogram, and electroencephalogram (EEG).
共有18名GBM患者参与了我们的前瞻性研究,评估生酮饮食疗法对肿瘤进展的影响,其中女性8名,男性10名,年龄介于34至75岁之间(中位年龄57.5岁)。这些患者来自我院及合作肿瘤科医生2016年1月至2021年7月期间的接诊病例,随访持续至2024年1月。本研究遵循1975年《赫尔辛基宣言》,并事先获得我校伦理委员会批准(编号PN 1232/16)。原计划采用双盲设计,但因疾病快速进展,将3年及以上生存期视为成功指标[30,31]。所有受试者均转诊至我院门诊进行神经学综合评估,包括神经状态检查和MRI评估。同时进行详细实验室检测,项目包括:全血细胞计数、生化检验(电解质、血糖、转氨酶、胆固醇、甘油三酯、甲状腺激素)、心电图及脑电图(EEG)。
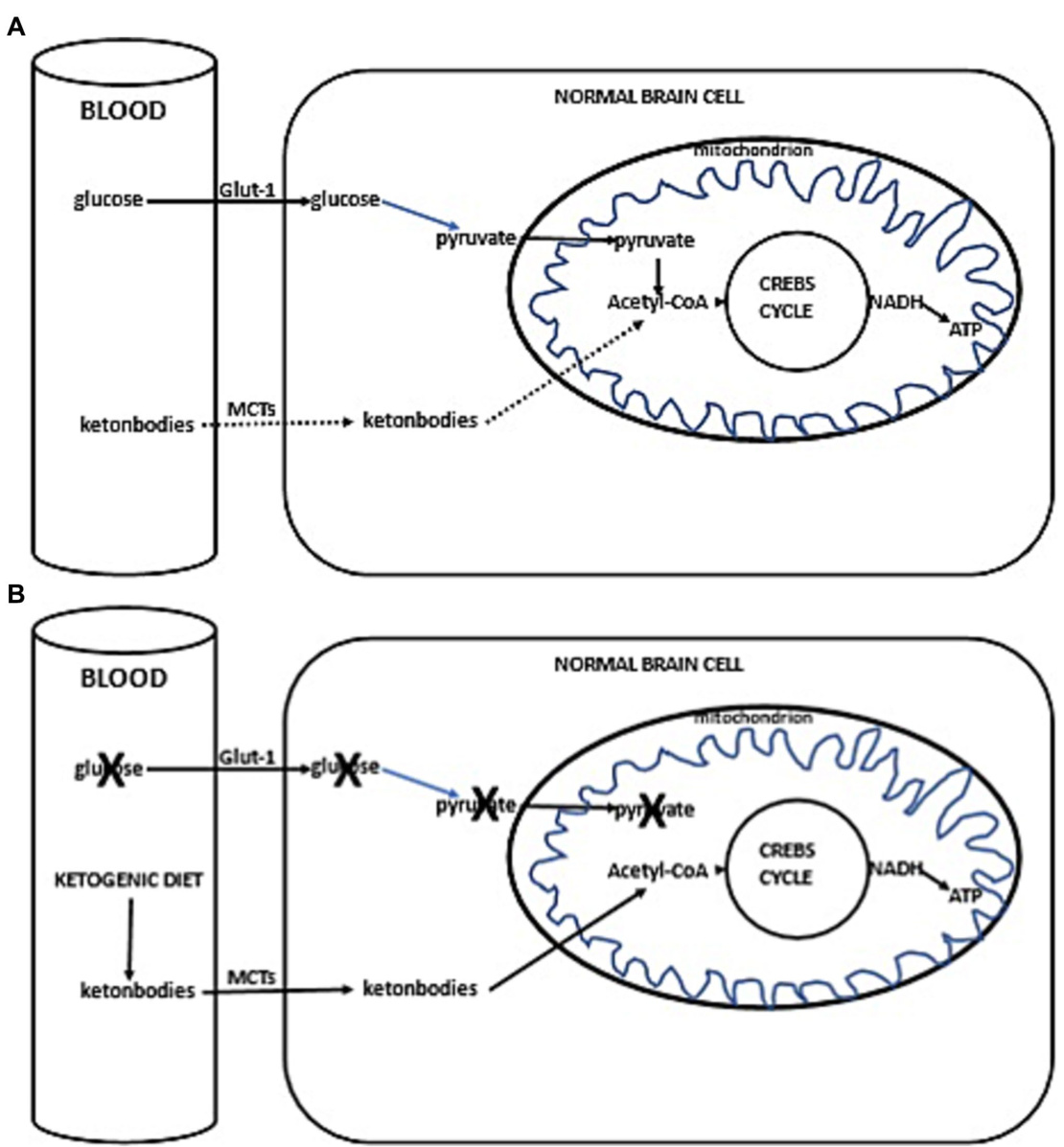
FIGURE 1 (A) Simplified scheme of glucose and ketone metabolism in a normal brain cell. Under anaerobic conditions, normal cells perform glycolysis in the cytoplasm, generating minimal but rapid energy. In aerobic conditions, normal cells perform the slower but more efficient oxidative phosphor yl ation in mitochondria for energy production. In a fed state, cellular energy is derived from glucose metabolism (illustrated with a solid line), undergoing glycolysis in the cytoplasm to form pyruvate, which then enters the mitochondrion. Inside the mitochondria, pyruvate is converted into acetyl-CoA, initiating the citric acid cycle (Krebs cycle), leading to the production of reducing equivalents. NADH/FADH are subsequently oxidized to generate ATP (solid line). In a fasted state, when glucose availability is low, the cell uses alternative ketone bodies that pass into the cell through mono carboxyl ate transporters (MCTs, indicated with a dotted line). Ketone bodies are converted into acetyl-CoA, prompting the citric acid cycle to proceed, similarly producing NADH (+H), which is oxidized to produce ATP (dotted line). (B) Ketogenic diet impact in normal brain cells. Due to the ketogenic dietinduced competition for available glucose, the primary source of acetyl-CoA switches to ketone bodies. These ketone bodies enter the cell via MCTs, leading to the production of acetyl-CoA. This initiates the citric acid cycle (Krebs cycle), resulting in the generation of NADH (+H). NADH is then oxidized, producing ATP.
图 1: (A) 正常脑细胞中葡萄糖和酮体代谢的简化示意图。在无氧条件下,正常细胞在细胞质中进行糖酵解,产生少量但快速的能量。在有氧条件下,正常细胞在线粒体中进行速度较慢但效率更高的氧化磷酸化以产生能量。在进食状态下,细胞能量来源于葡萄糖代谢(用实线表示),通过在细胞质中进行糖酵解形成丙酮酸,随后进入线粒体。在线粒体内,丙酮酸转化为乙酰辅酶A,启动三羧酸循环(Krebs循环),产生还原当量。NADH/FADH随后被氧化生成ATP(实线)。在禁食状态下,当葡萄糖供应不足时,细胞利用通过单羧酸转运体(MCTs,用虚线表示)进入细胞的替代性酮体。酮体转化为乙酰辅酶A,推动三羧酸循环进行,同样产生NADH(+H),其被氧化生成ATP(虚线)。(B) 生酮饮食对正常脑细胞的影响。由于生酮饮食引起对可用葡萄糖的竞争,乙酰辅酶A的主要来源转变为酮体。这些酮体通过MCTs进入细胞,导致乙酰辅酶A的产生。这启动了三羧酸循环(Krebs循环),产生NADH(+H)。NADH随后被氧化,生成ATP。
Each patient underwent a clinical assessment according to the ECOG (Eastern Cooperative Oncology Group) scale, before starting the ketogenic diet and every 3 months after. This scale is intended to assess how a patient’s disease is progressing, how the disease affects the daily living abilities, and to determine appropriate treatment and prognosis. Grade 0 means that the patient is fully active, able to carry pre-disease performance without restriction, while Grade 4 means that the patient is completely disabled; cannot perform any self-care; confined to bed or chair; in Grade 5, the patient is dead. Grades 2 and 3 are intermediary forms (32) (Table 1).
每位患者在开始生酮饮食前及之后每3个月按照ECOG (Eastern Cooperative Oncology Group) 量表进行临床评估。该量表用于评估患者疾病进展程度、疾病对日常生活能力的影响,并确定合适的治疗方案和预后。0级表示患者完全活动自如,能无限制地进行患病前的日常活动;4级表示患者完全丧失活动能力,无法进行任何自理活动,需卧床或坐轮椅;5级表示患者死亡。2级和3级为中间过渡状态 [32] (表 1)。
2.2 Inclusion–exclusion criteria
2.2 纳入-排除标准
Adult patients, 18–75 years old with newly diagnosed glioblastoma multiforme (GBM) were included. Patients with cachexia (weight body ${<}40\mathrm{kg}.$ , with severe cardiovascular or renal disease, and inherited metabolic disorders for which ketogenic diet is contra indicated, were excluded from the study.
纳入标准为18-75岁新确诊的多形性胶质母细胞瘤(GBM)成年患者。排除标准包括恶病质(体重<40kg)、严重心血管或肾脏疾病患者,以及生酮饮食禁忌的遗传性代谢疾病患者。
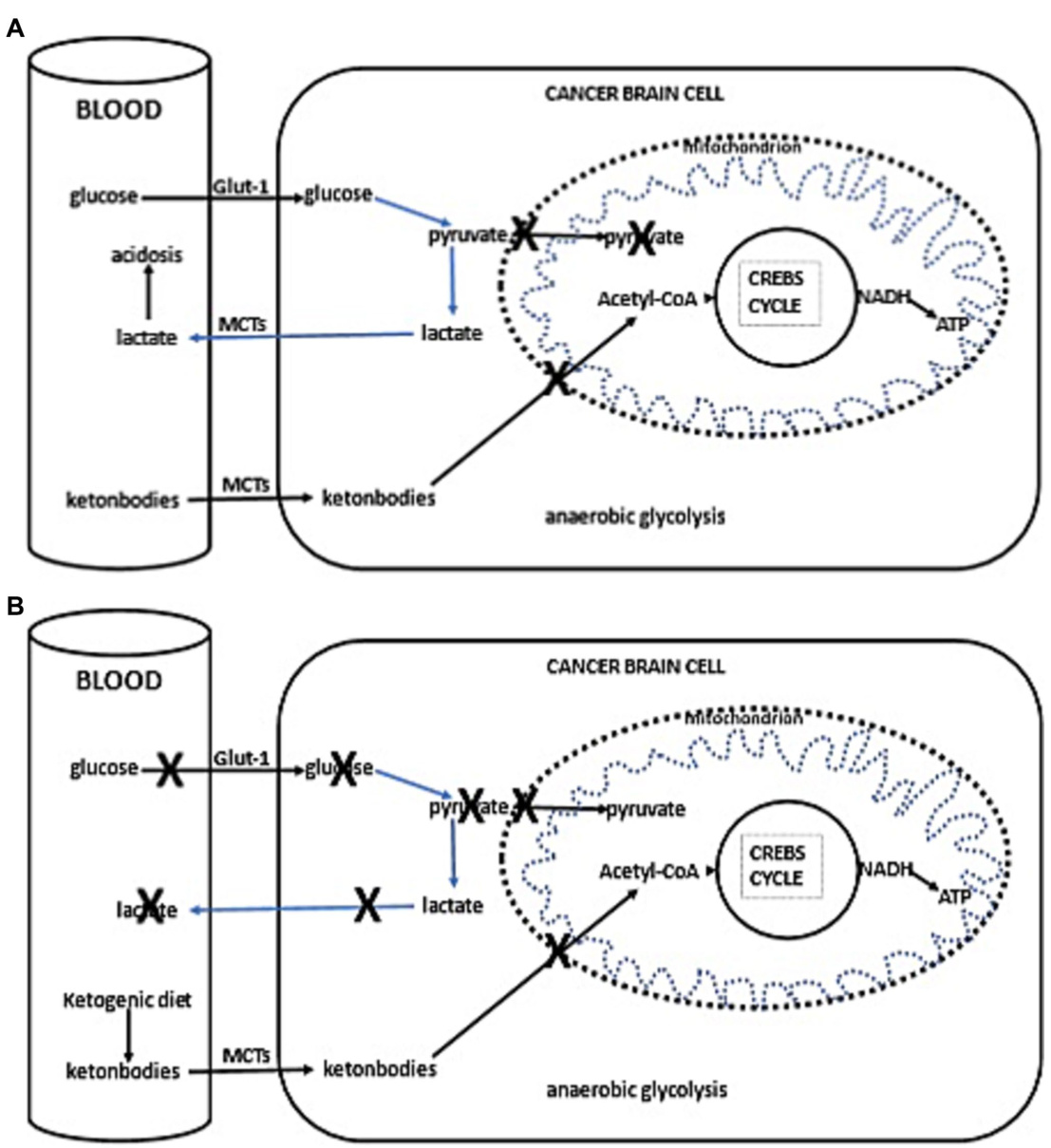
FIGURE 2 (A) Simplified schema of glucose and fat metabolism in a cancer cells. In addition to their reliance on glycolysis, most tumors, including those in the brain, exhibit abnormalities in the number and function of their mitochondria. Functional mitochondria are essential for utilizing ketones as an energy source. Consequently, for malignant cells, glycolysis becomes the primary source of ATP through the Embden–Meyerhof–Parnas pathway, regardless of oxygen availability. This glycolytic process is much less efficient than oxidative phosphor yl ation, as it generates less ATP per glucose molecule metabolized. Thus, conversion of glucose into lactic acid, bypassing oxidative phosphor yl ation, leads to reduced ATP production. To fulfill the elevated energy needs necessary for rapid tumor growth, cancer cells escalate glycolytic activity. The accumulation of lactate in cancer cells promotes lactate transport to the blood and extracellular fluid via proton-linked MCTs. This accumulation of lactic acid contributes to acidosis in both the blood and extracellular spaces, promoting ang io genesis, metastasis, and notably, immunosuppression, which is associated with worse clinical prognosis. (B) Ketogenic diet impact in cancer cells. The adoption of the ketogenic diet leads to an increase in hepatic keto genesis, which in turn inhibits glucose uptake by cells, positioning ketones as the primary energy substrate. However, the reduced ability of cancer cells to oxidize ketones efficiently, compounded by glucose deprivation, may result in reduced proliferation rates.
图 2: (A) 癌细胞中葡萄糖和脂肪代谢的简化示意图。除依赖糖酵解外,大多数肿瘤(包括脑部肿瘤)的线粒体数量和功能均存在异常。功能性线粒体是利用酮体作为能量来源的关键。因此,无论氧气供应是否充足,恶性细胞都主要通过 Embden-Meyerhof-Parnas 途径将糖酵解作为 ATP 的主要来源。与氧化磷酸化相比,该糖酵解过程效率低得多,因为每代谢一个葡萄糖分子产生的 ATP 更少。因此,绕过氧化磷酸化将葡萄糖转化为乳酸会导致 ATP 生成减少。为满足肿瘤快速生长所需的高能量需求,癌细胞会增强糖酵解活性。癌细胞中乳酸的积累会促进乳酸通过质子偶联的 MCTs 转运至血液和细胞外液。这种乳酸积累会导致血液和细胞外空间酸中毒,促进血管生成、转移,尤其是与不良临床预后相关的免疫抑制。(B) 生酮饮食对癌细胞的影响。采用生酮饮食会增加肝脏生酮作用,从而抑制细胞对葡萄糖的摄取,使酮体成为主要能量底物。然而,癌细胞氧化酮体的能力降低,再加上葡萄糖剥夺,可能导致增殖速率下降。
2.3 Ketogenic diet administration
2.3 生酮饮食干预
Following this enrollment evaluation, consultation was done by a clinical dietician and then, if the patient agreed to participate, the ketogenic diet was initiated. Prior to initiating the diet, comprehensive hematological and biochemical testing was conducted. This included, among other evaluations, a full blood count, a complete lipid profile, and purine levels to prevent the risk of gout. We started with a 1:1 diet (fat: protein $^{+}$ carbohydrates), and gradually, while monitoring ketonemia and glycemia, increased the ratio with the goal of reaching a 3:1 ratio, aiming for ketone values $>3.5\mathrm{mM/L}$ and glucose values ${<}80\mathrm{mg/dL}$ . Energy requirements were calculated based on the patients’ body weight at the time we took them on, using the Mifflin-St Jeor equation (which uses the current body weight). Our goal was not weight loss during the phase of standard therapy in these oncology patients However, we did observe that patients on the ketogenic diet initially lost weight and then stabilized. Thus, energy needs were calculated to maintain weight, though as previously mentioned, patients initially lost weight (on average $3{-}5\mathrm{kg}$ ), regardless of minor increases in caloric intake. The highest ketogenic ratio we reached was around 2.5:1 since, in adults, achieving a higher ketogenic ratio while meeting daily protein requirements is challenging; these requirements were calculated to provide $0.95{-}1.2\mathrm{g}/\mathrm{kg}/\mathrm{day}$ . We did not apply caloric restriction for our patients,. Besides, we did not have obese patients, only a few who were overweight. The diet was adapted to Mediterranean diet patterns due to the patient’s aggravated status from the disease itself and standard treatments, with the intention of avoiding additional side effects. The Mediterranean ketogenic diet, unlike the western ketogenic diet that uses saturated fatty acids as a source of fat, is based mainly on olive oil and other mono and polyunsaturated fatty acid sources (olives, avocado, nuts, ω-3 rich fish) and emphasizes the consumption of ω-rich fish and seafood as a source of protein. This dietary pattern is milder than the classic North American-Northwestern. An example of the diet applied is shown in Table 2.
在完成入组评估后,由临床营养师进行咨询。若患者同意参与,则开始生酮饮食。启动饮食方案前,我们进行了全面的血液学和生化检测,包括全血细胞计数、完整血脂谱及嘌呤水平检测以预防痛风风险。
初始采用1:1饮食比例(脂肪:蛋白质$^{+}$碳水化合物),通过监测血酮和血糖水平逐步提高比例,目标达到3:1比例,使血酮值$>3.5\mathrm{mM/L}$且血糖值${<}80\mathrm{mg/dL}$。能量需求根据患者入组时的体重采用Mifflin-St Jeor公式(基于当前体重)计算。
对于这些肿瘤患者的标准治疗阶段,我们的目标并非减重。但观察到生酮饮食患者初期体重下降后趋于稳定。因此尽管能量计算以维持体重为目标,患者初期仍平均减重$3{-}5\mathrm{kg}$(与热量摄入轻微增加无关)。成人因需满足每日$0.95{-}1.2\mathrm{g}/\mathrm{kg}$蛋白质需求,我们达到的最高生酮比例约为2.5:1。
未对患者实施热量限制,且入组患者中仅有少数超重者。考虑到疾病本身和标准治疗导致的健康恶化,饮食方案调整为地中海模式以避免额外副作用。与使用饱和脂肪酸的西方生酮饮食不同,地中海生酮饮食主要以橄榄油等单不饱和/多不饱和脂肪酸(橄榄、牛油果、坚果、富含ω-3的鱼类)为基础,并强调摄入富含ω的鱼类和海鲜作为蛋白质来源。该饮食模式比经典的北美-西北欧方案更温和。具体饮食示例见表2。
TABLE 1 Characteristics of all patients who participated in the study.
| P | G | A | DD | DS-TOO | Chemo + Rad prior KD administration | MB |
| 1 | M | 41 | 29/12/16 | 4/1/17 Total resection | 30 cycles of radiation (02/17) Temozolamide | IDH1(-) |
| 2 | M | 56 | 28/05/20 | 5/6/20 Total resection | 30 cycles of radiation (08/20) Temozolamide | IDH1(-) |
| 3 | F | 64 | 19/04/21 | 26/4/21 Total resection | 30 cycles of radiation (05/21) Temozolamide | IDH1(-) |
| 4 | M | 61 | 22/02/18 | 13/3/18 Stereotactic biopsy | 30 cycles of radiation (04/18) Temozolamide | IDH1(-) |
| 5 | M | 48 | 24/04/20 | 4/5/20 Total resection | 30 cycles of radiation (06/20) Temozolamide | IDH1(-) |
| 6 | M | 58 | 08/05/20 | 20/5/20 Total resection | 30 cycles of radiation (07/20) Temozolamide | IDH 1-2(-) |
| 7 | M | 60 | 11/12/18 | 19/12/18 Subtotal resection | 30 cycles of radiation (02/19) Temozolamide | IDH 1-2 (-) |
| 8 | M | 69 | 15/03/17 | 23/03/17 Total resection | 30 cycles of radiation (05/17) Temozolamide | IDH 1 (-) |
| 9 | M | 53 | 1/10/20 | 15/10/20 Subtotal resection | 30 cycles of radiation (11/20) Temozolamide | IDH 1 (-) |
| 10 | F | 57 | 16/02/21 | 26/2/21 Total resection | 30 cycles of radiation (04/21) Temozolamide | IDH1 (-) |
| 11 | F | 36 | 20/01/18 | 25/11/18 Subtotal resection | 30 cycles of radiation (02/19) Temozolamide | IDH1 (+) |
| 12 | F | 44 | 08/09/17 | 19/9/17 Total resection | 30 cycles of radiation (11/17) Temozolamide | IDH1 (+) |
| 34 | 24/07/20 | 3/8/20 Total resection | 30 cycles of radiation (10/20) Temozolamide | IDH 1-2 (-) | ||
| 16 | ||||||
| 17 | F | 59 | 04/04/19 | |||
| IDH 1 (-) | ||||||
| M | 71 | 22/01/20 | 24/2/20 | 30 cycles of radiation (04/20) | ||
| 14 | ||||||
| F | 59 | |||||
| 08/01/16 | IDH 1-2 (-) | |||||
| 22/1/16 | 30 cycles of radiation (03/16) | |||||
| Subtotal resection | ||||||
| Temozolamide | ||||||
| 15 | M | 51 | 02/05/19 | 16/5/19 | 30 cycles of radiation (06/19) | IDH 1-2 (-) |
| Total resection | Temozolamide | |||||
| F | 75 | 15/07/21 | 29/7/21 | 30 cycles of radiation (09/21) | IDH 1 (-) | |
| Total resection | Temozolamide | |||||
| 8/5/19 | 30 cycles of radiation (06/19) | IDH 1-2 (-) | ||||
| Subtotal resection | Temozolamide | |||||
| 18 |
Patients 1–6 (bold letters) are those who maintained the diet beyond 6 months. P, Patient; G, Gender; A, Age; DD, Diagnosis date; DS-TOO, Date of surgery-type of operation; Chemo $+\mathrm{Rad}$ , Chemotherapy $^+$ Radiation; KD, ketogenic diet; MB, Molecular biology.
表 1: 参与研究的所有患者特征。
| P | G | A | DD | DS-TOO | Chemo + Rad prior KD administration | MB |
|---|---|---|---|---|---|---|
| 1 | M | 41 | 29/12/16 | 4/1/17 Total resection | 30 cycles of radiation (02/17) Temozolamide | IDH1(-) |
| 2 | M | 56 | 28/05/20 | 5/6/20 Total resection | 30 cycles of radiation (08/20) Temozolamide | IDH1(-) |
| 3 | F | 64 | 19/04/21 | 26/4/21 Total resection | 30 cycles of radiation (05/21) Temozolamide | IDH1(-) |
| 4 | M | 61 | 22/02/18 | 13/3/18 Stereotactic biopsy | 30 cycles of radiation (04/18) Temozolamide | IDH1(-) |
| 5 | M | 48 | 24/04/20 | 4/5/20 Total resection | 30 cycles of radiation (06/20) Temozolamide | IDH1(-) |
| 6 | M | 58 | 08/05/20 | 20/5/20 Total resection | 30 cycles of radiation (07/20) Temozolamide | IDH 1-2(-) |
| 7 | M | 60 | 11/12/18 | 19/12/18 Subtotal resection | 30 cycles of radiation (02/19) Temozolamide | IDH 1-2 (-) |
| 8 | M | 69 | 15/03/17 | 23/03/17 Total resection | 30 cycles of radiation (05/17) Temozolamide | IDH 1 (-) |
| 9 | M | 53 | 1/10/20 | 15/10/20 Subtotal resection | 30 cycles of radiation (11/20) Temozolamide | IDH 1 (-) |
| 10 | F | 57 | 16/02/21 | 26/2/21 Total resection | 30 cycles of radiation (04/21) Temozolamide | IDH1 (-) |
| 11 | F | 36 | 20/01/18 | 25/11/18 Subtotal resection | 30 cycles of radiation (02/19) Temozolamide | IDH1 (+) |
| 12 | F | 44 | 08/09/17 | 19/9/17 Total resection | 30 cycles of radiation (11/17) Temozolamide | IDH1 (+) |
| 34 | 24/07/20 | 3/8/20 Total resection | 30 cycles of radiation (10/20) Temozolamide | IDH 1-2 (-) | ||
| 16 | ||||||
| 17 | F | 59 | 04/04/19 | IDH 1 (-) | ||
| M | 71 | 22/01/20 | 24/2/20 | 30 cycles of radiation (04/20) | ||
| 14 | ||||||
| F | 59 | 08/01/16 | 22/1/16 Subtotal resection | 30 cycles of radiation (03/16) Temozolamide | IDH 1-2 (-) | |
| 15 | M | 51 | 02/05/19 | 16/5/19 Total resection | 30 cycles of radiation (06/19) Temozolamide | IDH 1-2 (-) |
| F | 75 | 15/07/21 | 29/7/21 Total resection | 30 cycles of radiation (09/21) Temozolamide | IDH 1 (-) | |
| 8/5/19 Subtotal resection | 30 cycles of radiation (06/19) Temozolamide | IDH 1-2 (-) |
患者1-6(加粗字体)为坚持生酮饮食超过6个月者。P,患者编号;G,性别;A,年龄;DD,确诊日期;DS-TOO,手术日期-手术类型;Chemo + Rad,化疗联合放疗;KD,生酮饮食;MB,分子生物学特征。
2.4 Assessment criterion: statistics
2.4 评估标准:统计
As an assessment criterion, we set an optimistic target for adherence to the ketogenic diet beyond 6 months. The six-month timeframe was arbitrarily chosen based on our previous experience with studies involving the implementation of the ketogenic diet, where it served as an indicator of adherence (33, 34). We considered the therapeutic combination successful if the survival from diagnosis reached at least 3 years. The patients self-measured their blood glucose and ketone levels with blood glucose and $\beta$ -ketone test strips, in the morning and afternoon prep rand i ally. Initially, they did this daily for the first month and then twice a week. The readings were kept and referred to the dietitian with the diet records.
作为评估标准,我们设定了一个乐观目标:生酮饮食坚持超过6个月。选择六个月时间框架是基于我们以往实施生酮饮食研究的经验,该时长曾被用作依从性指标 [33, 34]。若患者从确诊起存活至少3年,我们则认为这种治疗组合是成功的。患者使用血糖和$\beta$-酮体试纸自行测量晨间及午后的血糖与酮体水平,最初第一个月每日监测,之后改为每周两次。所有读数记录均与饮食日志一并保存并提交给营养师参考。
TABLE 2 Example of ketogenic diet 2,150 Kcal 2:1 ratio.
| Morning | Snack | Lunch | Snack | Dinner |
| 17g tuna in oil | 20gfetacheese | 93g sardines | 1eggfortifiedwitho-3fatty acids | 117 g raw green salad |
| 60gketo-focaccia | 8golive oil | 41 g olive oil | 15g avocado | 93g salmon |
| 15 g tahini | 21 g olives | 117gboiledgreens | 9 g olive oil | 41 g olive oil |
| 14 g olive oil | 25g melon | |||
| 30g avocado |
Daily menu plan.
表 2: 生酮饮食示例 2,150 大卡 2:1 比例
| 早晨 | 零食 | 午餐 | 零食 | 晚餐 |
|---|---|---|---|---|
| 17克油浸金枪鱼 | 20克羊奶酪 | 93克沙丁鱼 | 1个富含ω-3脂肪酸的鸡蛋 | 117克生绿色沙拉 |
| 60克生酮佛卡夏 | 8克橄榄油 | 41克橄榄油 | 15克牛油果 | 93克三文鱼 |
| 15克芝麻酱 | 21克橄榄 | 117克水煮青菜 | 9克橄榄油 | 41克橄榄油 |
| 14克橄榄油 | 25克甜瓜 | |||
| 30克牛油果 |
每日菜单计划
Statistical analysis was done using the Statistical Analysis Systems statistical software package, version 20 (SAS Institute). Results were regarded as significant when $p<0.05$ . The difference between the two groups was assessed by the $t.$ -test for paired comparisons.
统计分析采用统计分析系统(Statistical Analysis Systems)统计软件包20版(SAS Institute)完成。当 $p<0.05$ 时认为结果具有统计学意义。两组间差异通过配对比较的 $t.$ 检验进行评估。
3 Cases presentation
3 案例展示
3.1 Patient 1: 84-months follow-up
3.1 病例1:84个月随访
A 41-year-old man was diagnosed with GBM of the left temporal lobe on December 2016 following a brain MRI (Figure 3). The presenting symptom was persistent headache and gradual wordfinding difficulty (anomic aphasia). He underwent surgical resection in January 2017, followed by 30 sessions of radiotherapy $(60\mathrm{Gy})$ along with chemotherapy (temozolomide). His to pathological examination was typical of GBM with IDH1-negative/MGMT-nonmethylated (Figure 4). On March 2017, the patient was started on a calorie restricted 1.4:1 ketogenic diet as adjunctive therapy (Table 3). Blood ketones and glucose levels were self-monitored daily. The patient achieved adequate ketosis during the first week of instituting the ketogenic diet and maintained high ketone levels $\left(3{-}4\mathrm{mmol/L}\right)$ and adequate blood glucose levels $\mathrm{(60-90~mg/dL)}$ ) throughout the observational period. The ketogenic diet was well tolerated, with only mild gastrointestinal side effects (constipation). In addition, he received temozolomide, initially dosed at $100\mathrm{mg/m^{2}/d a y}$ every other week. After 1 month, his dose increased to $200\mathrm{mg/m^{2}/d a y}$ on the same schedule, without toxicities. Temozolomide maintenance treatment lasted for 2 years. Serial MRI brain imaging was obtained every 4 months. His follow-up brain MRI 79 months after diagnosis shows no evidence of tumor recurrence (Figure 3). The patient reports a residual mild anomia and is currently working as a teacher. His most recent ECOG grade is 0.
一名41岁男性患者于2016年12月经脑部MRI (图3) 确诊为左颞叶胶质母细胞瘤 (GBM) 。主要症状为持续性头痛和渐进性命名障碍 (命名性失语) 。2017年1月接受手术切除,随后进行30次放疗 $(60\mathrm{Gy})$ 联合替莫唑胺化疗。病理检查显示典型IDH1阴性/MGMT非甲基化的GBM特征 (图4) 。2017年3月起,患者开始采用1.4:1热量限制生酮饮食作为辅助治疗 (表3) ,每日自行监测血酮和血糖水平。实施生酮饮食首周即达到理想酮症状态,并在整个观察期间维持较高酮体水平 $\left(3{-}4\mathrm{mmol/L}\right)$ 和正常血糖范围 $\mathrm{(60-90~mg/dL)}$ 。该饮食方案耐受性良好,仅出现轻微胃肠道副作用 (便秘) 。同步接受替莫唑胺治疗,初始剂量为隔周 $100\mathrm{mg/m^{2}/d a y}$ ,1个月后按相同方案增至 $200\mathrm{mg/m^{2}/d a y}$ ,未出现毒性反应。替莫唑胺维持治疗持续2年,每4个月进行系列脑部MRI复查。确诊79个月后的随访MRI显示无肿瘤复发迹象 (图3) 。患者目前遗留轻度命名障碍,从事教师职业,最新ECOG评分为0级。
3.2 Patient 2: 43-months follow-up
3.2 病例2:43个月随访
Patient 2 is a 59-year-old male. He is a primary school teacher in very good general condition, with a lean and athletic build (marathon runner). On 23/05/2020, at the age of 56, he was hospitalized due to persistent headache and a sudden onset of left hemi pares is, confusion, and vomiting. Brain CT showed a space-occupying right parietal– temporal lesion with solid and cystic elements and peripheral enhancement, as well as large perifocal edema with midline shift of $12\mathrm{mm}$ . A subsequent brain MRI (Figure 5) showed a large heterogeneous mass in the right tempor o parietal area, $53\mathrm{mm}$ in diameter, with hemorrhagic and necrotic elements and peripheral gadolinium enhancement, surrounded by extensive vasogenic edema. These radiological features were highly suggestive for GBM. On $05/06/2020$ , he underwent a total resection of the tumor through a right temporal craniotomy. He was discharged with le vet i race tam $1{,}000~\mathrm{mg}$ $\times2/$ day and methyl pre dni sol one per os in gradual tapering. His to logical examination (Figure 4) confirmed GBM, immuno his to chemically negative for IDH-1 mutation (GBM NOS). On 28/06/2020 he suffered a lower extremity deep vein thrombosis (DVT) and was placed on a therapeutic dose of heparin for 8 months. The patient followed 30 cycles of radiation (21/7/2020–31/8/2020) and was placed on temozolomide $150:\mathrm{mg/m}^{2}$ , 5 days/month, which continues until the present day. A classic ketogenic diet was implemented on 19/8/2020 with a ketogenic ratio $>2{:}1$ and a total daily calorie intake of $2,150\mathrm{kcal}$ (Table 3).
患者2为59岁男性,小学教师,总体健康状况良好,体型精瘦且运动型(马拉松跑者)。2020年5月23日(56岁时)因持续头痛伴突发左侧偏瘫、意识混乱及呕吐入院。脑部CT显示右顶颞叶占位性病变,含实性与囊性成分及周边强化,伴大面积瘤周水肿(中线移位达12mm)。后续脑部MRI(图5)显示右颞顶区存在53mm直径的异质性肿块,含出血坏死成分及周边钆剂强化,周围伴广泛血管源性水肿,影像学特征高度提示胶质母细胞瘤(GBM)。2020年6月5日行右颞开颅肿瘤全切术,出院时服用左乙拉西坦1,000mg(每日两次)并逐步减量口服甲泼尼龙。组织学检查(图4)确诊为IDH-1突变阴性的GBM(非特指型)。2020年6月28日出现下肢深静脉血栓(DVT),接受治疗剂量肝素治疗8个月。患者完成30次放疗(2020年7月21日–8月31日)后持续服用替莫唑胺(150mg/m²,每月5天)至今。2020年8月19日开始实施经典生酮饮食(生酮比>2:1,每日总热量摄入2,150kcal)(表3)。
The patient achieved satisfactory ketosis as early as the 1st week of diet initiation, with blood ketone levels of $2.9{-}5~\mathrm{mmol/L}$ and morning blood sugar of approximately $72{-}75\mathrm{mg/dL}$ . Nutritional ketosis is maintained until today. Close monitoring with serial MRIs shows no evidence of GBM recurrence throughout the observation period of 43 months (Figure 5). The patient is fully ambulatory, still working as a primary school teacher, with no imaging or clinical signs of disease activity. His most recent ECOG grade is 0.
患者在开始饮食治疗的第1周就达到了理想的酮症状态,血酮水平为$2.9{-}5~\mathrm{mmol/L}$,晨间血糖约为$72{-}75\mathrm{mg/dL}$。营养性酮症状态持续至今。通过连续MRI密切监测显示,在43个月的观察期内未出现胶质母细胞瘤(GBM)复发迹象(图5)。患者行动完全自如,仍担任小学教师工作,影像学及临床表现均无疾病活动征象。其最近一次ECOG评分为0级。
3.3 Patient 3: 33 months follow-up
3.3 患者3:33个月随访
A 65-year-old female was diagnosed with GBM in April 2021. Her presenting symptom was anomic aphasia. Brain MRI was remarkable for a space-occupying lesion at the left temporal lobe with he t erogenous signal on T2 sequences and irregular enhancement surrounded by large vasogenic oedema, consistent with GBM (Figure 6). Her his to pathological examination confirmed IDH1-negative GBM (Figure 4). She underwent surgery (total resection of the tumor) followed by radiotherapy—a total of 60 Gy in 30 RTs - and maintenance chemotherapy with temozolomide $120\mathrm{mg/m^{2}/d a y,}$ for 5 days each month. Ketogenic diet with a ketogenic ratio of $>2:1$ and total daily calorie intake of 1,500 kcal/day was introduced in July of the same year (Table 3). After 6 months the patient decided to abandon the diet due to perceived dietary restrictive ness. On April 2022, 4 months after KD discontinuation, GBM recurrence was followed by stereo tactic radio surgery (CyberKnife) (Figure 6). She also initiated second line chemotherapy with bevacizumab $(5{-}7\mathrm{mg/kg)}$ and irinotecan $120\mathrm{mg/}$ $\mathrm{m}^{2}$ twice/month, which is maintained until the present day. After relapse, the patient agreed to reinitiate the diet with improved adherence. Blood glucose levels were maintained between 75 and $85\mathrm{mg/dL}$ and ketone levels between 2 and 3 mmol/L. Her present ECOG grade is 0.
一名65岁女性于2021年4月被诊断为胶质母细胞瘤(GBM),首发症状为命名性失语。脑部MRI显示左颞叶占位性病变,T2序列呈不均匀信号伴不规则强化及周围大面积血管源性水肿,符合GBM表现(图6)。组织病理学检查确诊为IDH1阴性GBM(图4)。患者接受肿瘤全切手术后,进行了30次总剂量60Gy的放疗,并采用替莫唑胺维持化疗(120mg/m²/天,每月连用5天)。同年7月开始生酮饮食(生酮比>2:1,每日总热量摄入1500kcal)(表3)。6个月后患者因感觉饮食限制过多而中止该方案。2022年4月(停用生酮饮食4个月后)肿瘤复发,遂接受立体定向放射外科治疗(CyberKnife)(图6),并开始二线化疗方案:贝伐珠单抗(5-7mg/kg)联合伊立替康(120mg/m²,每月两次),该方案持续至今。复发后患者同意重新开始生酮饮食且依从性提高,血糖维持在75-85mg/dL,血酮水平维持在2-3mmol/L。目前ECOG评分为0分。
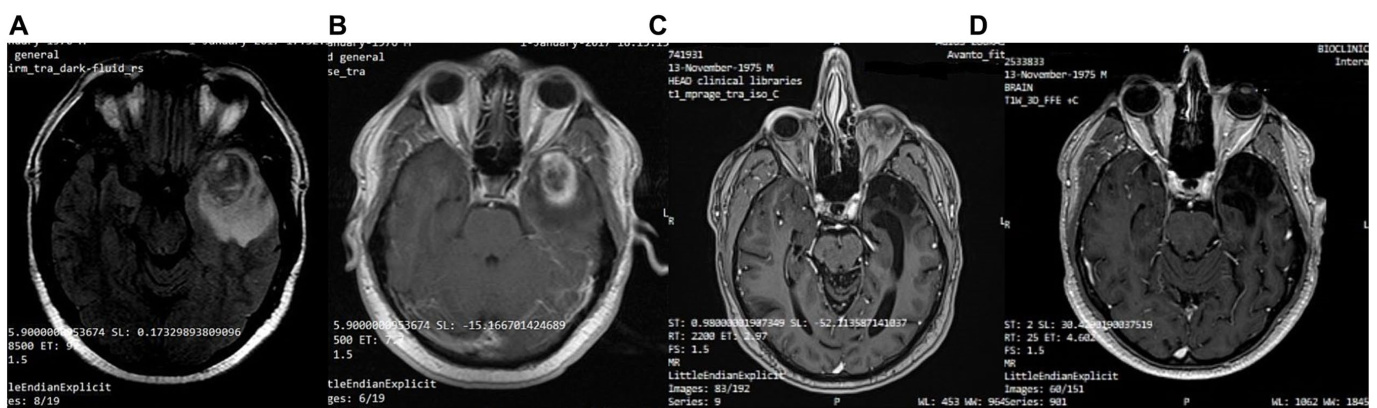
FIGURE 3 Patient 1: (A) Pre-operative brain MRI (T2/FLAIR) (B) Pre-operative brain MRI (T1 with contrast) (C) 38-month follow-up brain MRI (T1 with contrast) (D) 80-month follow-up brain MRI (T1 with contrast).
图 3: 患者1: (A) 术前脑部MRI (T2/FLAIR) (B) 术前脑部MRI (T1增强) (C) 38个月随访脑部MRI (T1增强) (D) 80个月随访脑部MRI (T1增强)。
3.4 Patient 4: 43-month follow-up
3.4 病例4:43个月随访
A 63-year-old man was diagnosed in February 2018 with GBM following a first epileptic seizure. The patient experienced an episode of focal seizures involving the right upper and lower limb. On neurological examination, a mild right-sided hemi pares is was noted. Brain MRI revealed a large heterogeneous ly enhancing tumor in the left parietal lobe with a central nodule and surrounding vasogenic oedema, extending through the corpus callosum to the contra lateral side (Figure 7). An EEG demonstrated paroxysmal activity consisting of intermittent sharp theta waves on the left fronto central region and the patient was put on le vet i race tam. Stereo tactic brain biopsy and his to pathological examination confirmed IDH1-negative GBM (Figure 4). The patient was considered inoperable due to the extent of the tumor, which infiltrated the corpus callosum and extended across the midline. The patient received radiotherapy (30 sessions, 60 Gy in total) along with chemotherapy (temozolomide) and corticosteroids (dex amet has one per os). A 3:1 ketogenic diet was initiated in April 2018 just before radiotherapy (Table 3). After radiation therapy, corticosteroids were gradually withdrawn and the patient was maintained on a treatment regimen of $250\mathrm{mg}$ temozolomide in total per day for 5 days every 4 weeks (until July 2019), alongside ketogenic diet therapy. The diet was well-tolerated, and the patient achieved and maintained ketosis (ketonemia $3{-}4\mathrm{mmol/L}$ ) and lower blood glucose levels $(70{-}85\mathrm{mg/dL})$ throughout the follow-up period. Brain MRI was performed every 3 months showing no tumor progression and less surrounding vasogenic oedema, while the enhancing nodule in the left semioval center was decreasing with minor enhancement (Figure 7).
2018年2月,一名63岁男性首次癫痫发作后被诊断为胶质母细胞瘤(GBM)。患者出现累及右上肢和右下肢的局灶性癫痫发作。神经系统检查发现轻度右侧偏瘫。脑部MRI显示左顶叶存在一个大型异质性强化肿瘤,中央有结节并伴有周围血管源性水肿,肿瘤通过胼胝体延伸至对侧 (图7)。脑电图显示左额中央区出现阵发性间歇性尖θ波活动,患者开始服用左乙拉西坦。立体定向脑活检及组织病理学检查确诊为IDH1阴性胶质母细胞瘤 (图4)。由于肿瘤范围广泛,已浸润胼胝体并跨越中线,患者被判定为无法手术。患者接受了放疗(30次,总剂量60Gy)联合化疗(替莫唑胺)及皮质类固醇治疗(口服地塞米松)。2018年4月放疗前开始采用3:1生酮饮食 (表3)。放疗结束后逐渐停用皮质类固醇,并维持每4周服用5天(每日总量$250\mathrm{mg}$)替莫唑胺的治疗方案(持续至2019年7月),同时配合生酮饮食疗法。患者对饮食方案耐受良好,在整个随访期间保持酮症状态(血酮$3{-}4\mathrm{mmol/L}$)及较低血糖水平$(70{-}85\mathrm{mg/dL})$。每3个月进行的脑部MRI显示肿瘤无进展且周围血管源性水肿减轻,同时左半卵圆中心强化结节逐渐缩小且强化程度减弱 (图7)。
However, 32 months after diagnosis, the patient suffered a GBM relapse (Figure 7). While continuing the ketogenic diet, he underwent surgical resection and was put on second line chemotherapy with bevacizumab $(5{-}7\mathrm{mg/kg})$ and irinotecan $\mathrm{120~mg/m^{2}},$ ) until his death in September 2021 (43 months post-diagnosis).
然而,确诊32个月后,患者出现胶质母细胞瘤复发 (图 7)。在坚持生酮饮食的同时,他接受了手术切除,并开始使用贝伐珠单抗 $(5{-}7\mathrm{mg/kg})$ 和伊立替康 $\mathrm{120~mg/m^{2}}$ 进行二线化疗,直至2021年9月去世 (确诊后43个月)。
3.5 Patient 5: 44 months follow-up
3.5 患者5:44个月随访
A 48-year-old male guitar teacher presented at the emergency department in April 2020 with confusion, agitation, anomic aphasia, and left hemi pares is. His symptoms developed gradually over a period of 1 month, during which he complained of frequent headaches. Brain
一名48岁男性吉他教师于2020年4月因意识模糊、躁动、命名性失语及左侧轻偏瘫就诊急诊科。症状在1个月内逐渐发展,期间主诉频繁头痛。脑部
MRI demonstrated a large contrast enhancing right hemispheric lesion expanding contra laterally through corpus callosum, as well as supra ten tori ally to the right cerebellum, with irregular borders, necrotic and hemorrhagic areas and vast peri lesion al vasogenic oedema (Figure 8). These features were consistent with GBM, as was later confirmed by his to pathological examination that showed grade IV IDH1-negative GBM (Figure 4). Ketogenic diet was introduced soon after diagnosis, as an adjunctive treatment to standard of care (tumor resection, radiotherapy, chemotherapy). Anti convulsive treatment (le vet i race tam) was also started due to focal aware motor seizures. The patient was put on classic ketogenic diet (ketogenic ratio of 2.5:1) with MCT supplement ation, with a total caloric intake of 2000 kcal/day, containing $189\mathrm{g/d}$ fat, $65~\mathrm{g/d}$ proteins, $11\mathrm{g}/\mathrm{d}$ carbohydrates and $_{3-4\mathrm{g}}$ MCT per meal (Table 3). The patient achieved and maintained ketosis (ketone levels $3{-}4\mathrm{mmol/L}$ ) and lower blood glucose levels $(70{-}85\mathrm{mg/dL})$ ) soon after KD initiation. As a side effect during KD, the patient reported chronic constipation that was relieved by conservative or p harm a co logical means. During follow-up, blood ketone levels oscillated between $2{-}3\mathrm{mmol/L}$ and blood glucose ranged from 80 to $90\mathrm{mg/dL}$ .
MRI显示右侧大脑半球有一处大型对比增强病灶,通过胼胝体向对侧扩展,并向上累及右侧小脑幕,边界不规则,伴有坏死、出血区域及广泛的病灶周围血管源性水肿 (图 8)。这些特征符合胶质母细胞瘤 (GBM) 表现,后续组织病理学检查证实为IDH1阴性IV级GBM (图 4)。确诊后立即在标准治疗(肿瘤切除、放疗、化疗)基础上引入生酮饮食作为辅助疗法。由于出现局灶性意识清醒型运动性癫痫发作,同时开始抗惊厥治疗(左乙拉西坦)。患者采用经典生酮饮食(生酮比例2.5:1)并补充中链甘油三酯(MCT),每日总热量摄入2000千卡,包含脂肪189g/d、蛋白质65g/d、碳水化合物11g/d,每餐添加3-4g MCT (表 3)。开始生酮饮食后患者迅速达到并维持酮症(酮体水平3-4mmol/L),血糖水平降低至70-85mg/dL。生酮期间出现慢性便秘副作用,通过保守或药物手段缓解。随访期间血酮水平波动于2-3mmol/L,血糖维持在80-90mg/dL范围。
The patient had no evidence of disease progression for almost 3 years, having a mild residual left hemi pares is and therefore being able to carry lighter everyday activities (ECOG grade 1). However, in May 2023 (36 months post diagnosis), the patient suffered a GBM recurrence (Figure 8) and was initiated with second line bevacizumab $(5{-}7\mathrm{mg/kg)}$ and irinotecan $(120\mathrm{mg/m}^{2^{*}}$ ) every other week. He is currently under CyberKnife treatment (4–5 sessions over 1–2 weeks). His present ECOG performance status is 3 (capable of only limited self-care; confined to bed or chair more than $50%$ of waking hours).
该患者在近3年内未出现疾病进展迹象,仅遗留轻度左侧偏瘫,因此能够从事较轻的日常活动 (ECOG 1级)。然而在2023年5月 (确诊后36个月),患者出现胶质母细胞瘤复发 (图8),开始接受二线贝伐珠单抗 $(5{-}7\mathrm{mg/kg})$ 联合伊立替康 $(120\mathrm{mg/m}^{2^{*}}$) 隔周治疗。目前正在接受射波刀治疗 (1-2周内4-5次疗程),现ECOG体能状态评分为3级 (仅能有限自理;清醒状态下超过 $50%$ 时间需卧床或坐椅)。
3.6 Patient 6: 36 months follow-up
3.6 病例6:36个月随访
A 58-year-old priest presented with neuro-psychiatric symptoms in April 2020, such as headaches, personality changes and aggressiveness. For this reason, he underwent a brain MRI, which revealed a space-occupying lesion on the left occipito-parietal region with heterogeneous enhancement (Figure 9). The patient underwent total excision of the tumor on May 20, 2020. His to logical examination demonstrated GBM immuno his to chemically negative for IDH-1&2 mutation (GBM
一位58岁的神职人员于2020年4月出现神经精神症状,包括头痛、性格改变和攻击性。为此,他接受了脑部MRI检查,结果显示左侧枕顶区存在不均匀强化的占位性病变(图9)。患者于2020年5月20日接受了肿瘤全切术。组织学检查显示为胶质母细胞瘤(GBM),免疫组化检测IDH-1&2突变呈阴性。
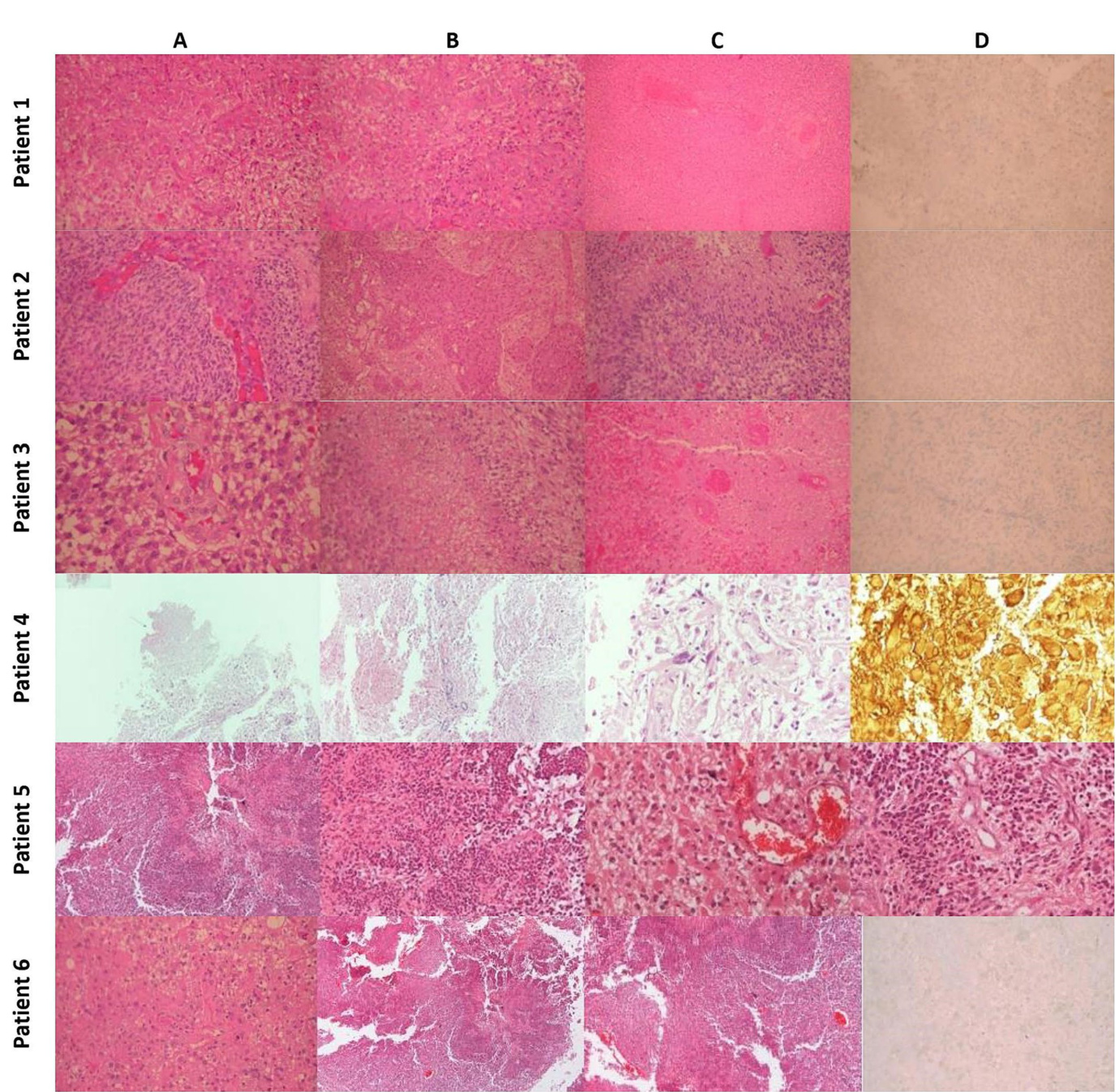
His to pathology: Patient 1 (A) Typical Morphology of Glioblastoma (H&E x200). (B) Significant endo the li al hyperplasia (H&E x200). (C) Extensive Coa gul at ive Necrosis with Thrombotic Vessels (H&E x100). (D) Tumor cells negative for IDH-1 Mutant (IHC x200). Patient 2: (A) Typical morphology of glioblastoma with endo the li al hyperplasia (H&E x200). (B) Severe endo the li al hyperplasia (X100). (C) Palisading necrosis (H&E x200). (D) Tumor cells are negative for IDH-1 mutant (IHC $\times200$ ). Patient 3 (A) Typical morphology of glioblastoma with endo the li al hyperplasia (H&E x200). (B) Palisading necrosis (H&E $\times200,$ ). (C) Extensive coa gul at ive necrosis with thrombotic vessels (H&E $\times200)$ . (D) Tumor cells are negative for IDH-1 mutant (IHC x200). Patient 4 (A) Region of tumor necrosis (H&Ex40). (B) Endo the li al hyperplasia (H&Ex100). (C) Ple om orphic glial cells (H&E $\times400;$ . (D) GFAP $^+$ neoplastic cells and gem is to cyte s (H&Ex400). Patient 5 (A) Region of tumor necrosis (H&E $\times40)$ ). (B) Neoplastic cells surrounding central necrosis (H&E x100). (C) Glial cells with gem is to cy tic features and micro vascular proliferation (H&E $\times200$ ). (D) Endo the li al hyperplasia and micro vascular proliferation (H&E $\times200)$ ). Patient 6 (A) Typical morphology of glioblastoma (H&E $\times200.$ ). (B) Area of geographic necrosis (H&E $\times200$ ). (C) Endo the li al hyperplasia (H&E $\times200)$ . (D) Tumor cells negative for IDH-1 Mutant (IHC $\times200,$ ).
病例1组织病理学: (A) 胶质母细胞瘤典型形态 (H&E ×200)。 (B) 显著内皮增生 (H&E ×200)。 (C) 广泛凝固性坏死伴血栓形成血管 (H&E ×100)。 (D) IDH-1突变阴性肿瘤细胞 (IHC ×200)。
病例2: (A) 伴内皮增生的胶质母细胞瘤典型形态 (H&E ×200)。 (B) 重度内皮增生 (×100)。 (C) 栅栏状坏死 (H&E ×200)。 (D) IDH-1突变阴性肿瘤细胞 (IHC ×200)。
病例3: (A) 伴内皮增生的胶质母细胞瘤典型形态 (H&E ×200)。 (B) 栅栏状坏死 (H&E ×200)。 (C) 广泛凝固性坏死伴血栓形成血管 (H&E ×200)。 (D) IDH-1突变阴性肿瘤细胞 (IHC ×200)。
病例4: (A) 肿瘤坏死区域 (H&E ×40)。 (B) 内皮增生 (H&E ×100)。 (C) 多形性胶质细胞 (H&E ×400)。 (D) GFAP⁺肿瘤细胞与双核细胞 (H&E ×400)。
病例5: (A) 肿瘤坏死区域 (H&E ×40)。 (B) 中央坏死周围肿瘤细胞 (H&E ×100)。 (C) 具双核特征的胶质细胞伴微血管增生 (H&E ×200)。 (D) 内皮增生与微血管增生 (H&E ×200)。
病例6: (A) 胶质母细胞瘤典型形态 (H&E ×200)。 (B) 地图状坏死区域 (H&E ×200)。 (C) 内皮增生 (H&E ×200)。 (D) IDH-1突变阴性肿瘤细胞 (IHC ×200)。
NOS). The patient then underwent 30 sessions of radiation therapy $(60\mathrm{Gy})$ in combination with temozolomide $(75~\mathrm{mg}/\mathrm{m}^{2})$ and dex amet has one. Subsequently, the patient received maintenance chemotherapy with temozolomide $150:\mathrm{mg/m}^{2}$ for 21 months (Figure 9). In November 2020, 6 months after the diagnosis, he started a classical ketogenic diet with a ketogenic ratio $>2.5{:}1$ (Table 3), which was well-tolerated, and the patient maintained low blood glucose levels $(75{-}90~\mathrm{mg/dL})$ and satisfactory ketosis.
随后,患者接受了30次放疗 $(60\mathrm{Gy})$ 联合替莫唑胺 $(75~\mathrm{mg}/\mathrm{m}^{2})$ 和地塞米松治疗。接着,患者继续接受替莫唑胺 $150:\mathrm{mg/m}^{2}$ 维持化疗21个月 (图 9)。2020年11月(确诊后6个月),他开始采用生酮比例 $>2.5{:}1$ 的标准生酮饮食 (表 3),耐受性良好,血糖水平维持在 $(75{-}90~\mathrm{mg/dL})$ 且酮症状态理想。
In February 2022, 22 months after the diagnosis, the patient experienced a focal epileptic seizure and was diagnosed with a recurrence of the GBM on a subsequent brain MRI (Figure 9). For this reason, he underwent 3 sessions of stereo tactic radiotherapy (CyberKnife), and the patient was placed on second-line chemotherapy with bevacizumab $(5{-}7\mathrm{mg/kg})$ and irinotecan $120~\mathrm{mg/}$ $\mathrm{m}^{2}$ twice a month. He continued the ketogenic diet but ultimately passed away from disease complications in May 2023, 36 months after the diagnosis.
2022年2月,即确诊22个月后,患者出现局灶性癫痫发作,后续脑部MRI检查确诊胶质母细胞瘤(GBM)复发(图9)。为此,他接受了3次立体定向放射治疗(CyberKnife),并开始二线化疗方案:贝伐珠单抗$(5{-}7\mathrm{mg/kg})$联合伊立替康$120~\mathrm{mg/}$$\mathrm{m}^{2}$,每两周给药一次。患者持续生酮饮食治疗,但最终于2023年5月因疾病并发症去世,距确诊36个月。
TABLE 3 Patient’s Ketogenic Diet: Total daily intake.
| Patient-KD | Duration | Kcal | Fat g/d | Protein g/d | CHOs g/d | KR |
| Patient 1 Modified Ketogenic Diet | 25.4.2017-present date | 2000 | 169 | 100 | 20 | 1.4: 1 |
| Patient 2 | 1st diet (19.8.2020) | 2,150 | 189.2 | 73.9 | 19.6 | >2: 1 |
| Mediterranean ketogenicdiet with MCTs* | 2nd diet (02.11.2021) | 2,195 | 201.7 | 73.9 | 19.6 | >2,2: 1 |
| 3rd diet | 2,298 | 213 | 75 | 20 | >2,2: 1 | |
| 05.7.2021 - present date 1,500 136 g/d 57 g/d 13 g/d | ||||||
| Mediterranean Ketogenic Diet | ||||||
| Patient 4. Mediterraneanketogenicdiet with | 1st diet (25.4.2018) | 2,000 | 181.9 | 73 | 17.6 | 2:1 |
| MCTs*. | 2nd diet (20.09.2019) | 2,125 | 195.5 | 73.2 | 18 | >2:1 |
| *The patient received >5gr of MCT oil before bedtime. | ||||||
| Patient 5 Mediterranean Ketogenic Diet | 27.4.2020 - present date | 2,000 | 189 g/d | P/8 s9 | 11 g/d | 2.5: 1 |
| Patient 6 | 08.11.2020 05.05.2023 | 2,000 | 166 g/d | 75 g/d | 25 g/d | >2.5: 1 |
Fats are based mainly on olive oil, avocado, olives, raw nuts and seeds and proteins derive mainly from fatty fish and chicken. MCTs, Medium-chain triglycerides; CHOs, Carbohydrates; KD, Ketogenic diet; KR, Ketogenic ratio.
表 3: 患者生酮饮食每日总摄入量
| 患者-KD | 持续时间 | 千卡 | 脂肪(克/天) | 蛋白质(克/天) | 碳水化合物(克/天) | 生酮比 |
|---|---|---|---|---|---|---|
| 患者1改良生酮饮食 | 2017年4月25日至今 | 2000 | 169 | 100 | 20 | 1.4:1 |
| 患者2 | 第一次饮食(2020年8月19日) | 2150 | 189.2 | 73.9 | 19.6 | >2:1 |
| 含MCTs*的地中海生酮饮食 | 第二次饮食(2021年11月2日) | 2195 | 201.7 | 73.9 | 19.6 | >2.2:1 |
| 第三次饮食 | 2298 | 213 | 75 | 20 | >2.2:1 | |
| 地中海生酮饮食 | 2021年7月5日至今 | 1500 | 136 | 57 | 13 | |
| 患者4. 含MCTs*的地中海生酮饮食 | 第一次饮食(2018年4月25日) | 2000 | 181.9 | 73 | 17.6 | 2:1 |
| 第二次饮食(2019年9月20日) | 2125 | 195.5 | 73.2 | 18 | >2:1 | |
| 患者5地中海生酮饮食 | 2020年4月27日至今 | 2000 | 189 | P/8 s9 | 11 | 2.5:1 |
| 患者6 | 2020年11月8日-2023年5月5日 | 2000 | 166 | 75 | 25 | >2.5:1 |
*患者睡前服用>5克MCT油。
脂肪主要来自橄榄油、牛油果、橄榄、生坚果和种子,蛋白质主要来自多脂鱼类和鸡肉。MCTs:中链甘油三酯;CHOs:碳水化合物;KD:生酮饮食;KR:生酮比。
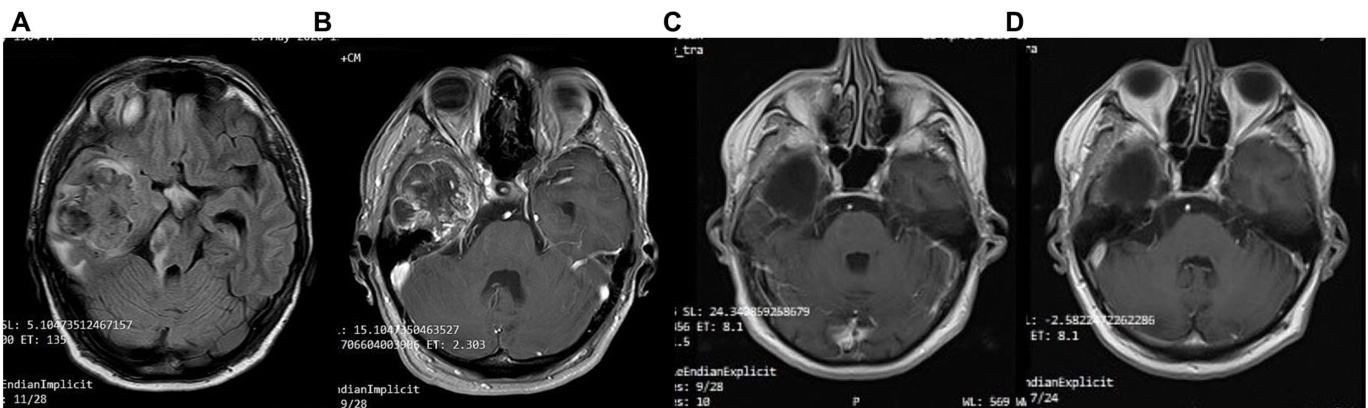
FIGURE 5 Patient 2: (A) pre-operative brain MRI (T2/FLAIR) (B) pre-operative brain MRI (T1 with contrast) (C) 20-month follow-up brain MRI (T1 with contrast) (D) 40-month follow-up brain MRI (T1 with contrast).
图 5 患者 2: (A) 术前脑部 MRI (T2/FLAIR) (B) 术前脑部 MRI (T1 增强) (C) 20 个月随访脑部 MRI (T1 增强) (D) 40 个月随访脑部 MRI (T1 增强)。
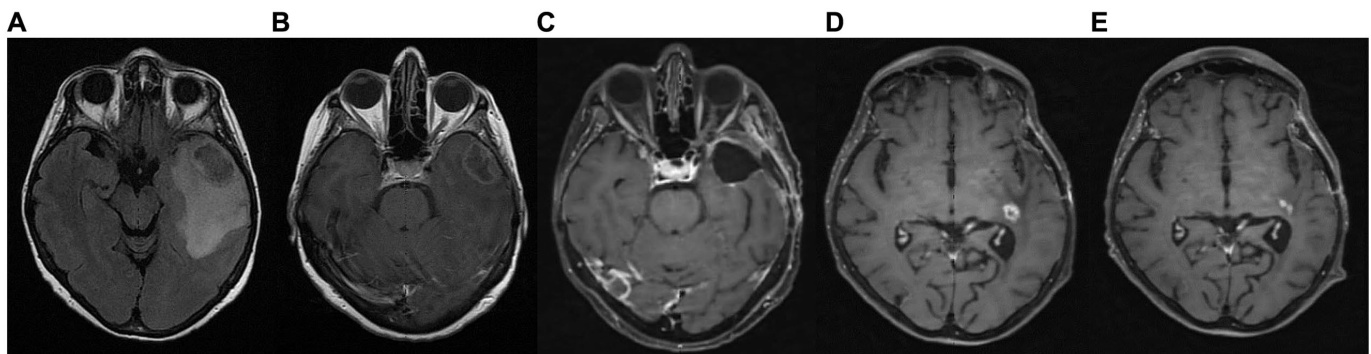
FIGURE 6 Patient 3: (A) brain MRI on diagnosis (T2/FLAIR) (B) brain MRI on diagnosis (T1 with contrast) (C) 9-month follow up brain MRI (T1 with contrast) (D) GBM relapse, 12-month follow up brain MRI (T1 with contrast) (E) 30-month follow up brain MRI (T1 with contrast).
图 6 患者3: (A) 确诊时脑部MRI (T2/FLAIR) (B) 确诊时脑部MRI (增强T1) (C) 9个月随访脑部MRI (增强T1) (D) GBM复发, 12个月随访脑部MRI (增强T1) (E) 30个月随访脑部MRI (增强T1)。
4 Results
4 结果
Out of the 18 patients, 6 followed the diet for more than 6 months (Figure 10). The effect of diet on the disease evolution of these patients is shown in Table 4. More specifically, from the 6 patients who followed the diet for more than 6 months, one patient died at 43 months (thus achieving 3 years survival), one patient died exactly 36 months after diet initiation (thus narrowly missing 3 years survival), and one patient is still alive 33 months after the start of the diet (but has not yet reached the 3-year goal, and is not included in the final percentage). The remaining 3 are also still alive, completing 84, 43, and 44 months of life, respectively. Therefore, the 3-year survival rate .
在18名患者中,有6人坚持饮食疗法超过6个月 (图 10)。这些患者的饮食对疾病进展的影响如表 4所示。具体而言,在坚持饮食超过6个月的6名患者中:1名患者在43个月时去世(即实现3年生存),1名患者恰好在开始饮食疗法36个月后去世(以微弱差距未达3年生存目标),另1名患者在开始饮食33个月后仍存活(但尚未达到3年目标,故未计入最终百分比)。其余3名患者目前仍存活,分别完成84个月、43个月和44个月的生存期。因此,3年生存率为。
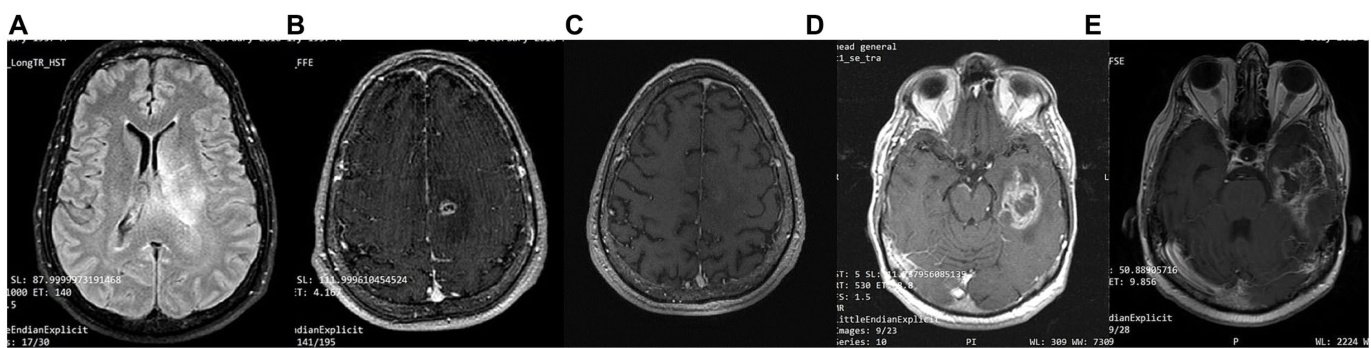
FIGURE 7 Patient 4: (A) brain MRI on diagnosis (T2/FLAIR) (B) brain MRI on diagnosis (T1 with contrast) (C) 24-month follow-up brain MRI (T1 with contrast) (D) 32-month follow up brain MRI. GBM relapse (T1 with contrast) (E) 41-month follow up brain MRI (T1 with contrast).
图 7: 患者4: (A) 确诊时脑部MRI (T2/FLAIR) (B) 确诊时脑部MRI (增强T1) (C) 24个月随访脑部MRI (增强T1) (D) 32个月随访脑部MRI。胶质母细胞瘤复发 (增强T1) (E) 41个月随访脑部MRI (增强T1)
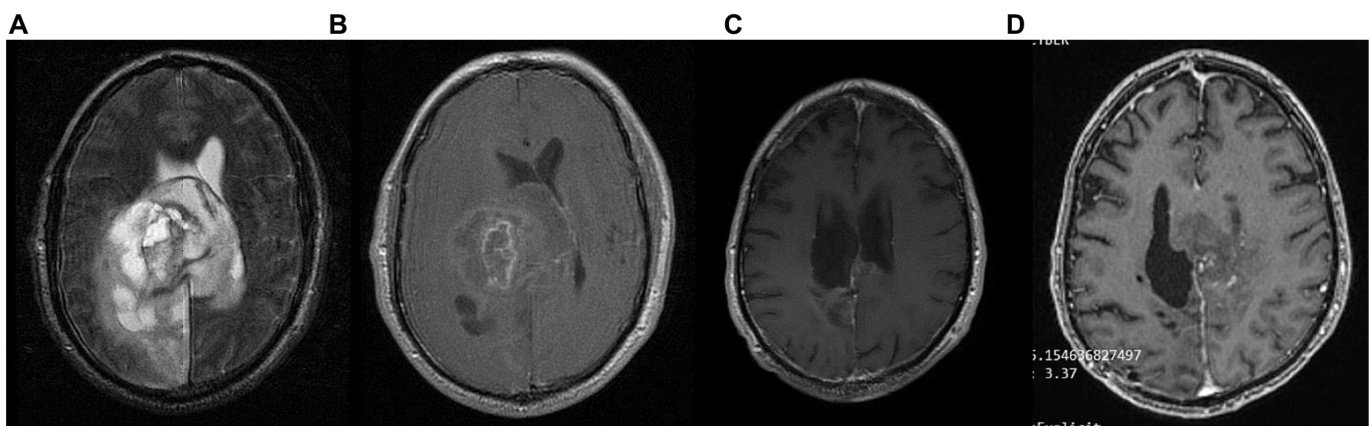
FIGURE 8 Patient 5: (A) pre-operative brain MRI (T2/FLAIR) (B) pre-operative brain MRI (T1 with contrast) (C) 34-month follow up brain MRI (T1 with contrast) (D) GBM relapse 40-month follow up brain MRI (T1 with contrast).
图 8 患者5: (A) 术前脑部MRI (T2/FLAIR) (B) 术前脑部MRI (T1增强) (C) 34个月随访脑部MRI (T1增强) (D) GBM复发40个月随访脑部MRI (T1增强)。
The characteristics of the patients who did not comply with the diet beyond 6 months are shown in Table 5. Of the 12 patients who did not adhere to the diet, only one reached 36 months of survival, while the rest have died in an average time of $15.7\pm6.7$ months, with a 3-year survival rate of $8.3%$ .
未坚持饮食超过6个月的患者特征如表5所示。在12名未遵守饮食方案的患者中,仅1例存活达到36个月,其余患者平均生存时间为$15.7\pm6.7$个月,3年生存率为$8.3%$。
Comparing the survival rates of the two groups, we see that the difference is $58.3%$ (66.7 versus $8.3%$ ) and is statistically significant with $p<0.05$ (0.0114) and $\mathrm{X}^{2}=6.409$ .
比较两组的存活率,我们发现差异为 $58.3%$ (66.7 对比 $8.3%$),且具有统计学显著性 ($p<0.05$) (0.0114) 以及 $\mathrm{X}^{2}=6.409$。
Unique features were observed in the 6 patients who adhered to the diet (Table 3). Patient 1 (P1) received a combination of radiation and $75:\mathrm{mg}/\mathrm{m}^{2}$ temozolomide for 1 month. He continued with maintenance temozolomide at $180:\mathrm{mg/m}^{2}$ , 5 days/month for 24 months and then discontinued it. In total, he received concurrent chemotherapy $+\mathrm{KD}$ for 24 months. Only KD was administered in the remaining observation time (60 months). His ECOG performance status was excellent with score 0 (fully active). Patient P2 is alive at 43 months, with 36 months under ketogenic diet therapy with ECOG 1.Patient P3 stopped the ketogenic diet and relapsed soon after. She was initially treated with chemotherapy and cortisone without an increase in her blood glucose levels, and after the end of chemotherapy, she resumed the ketogenic diet and since then recovered with ECOG 1. All 6 patients received chemotherapy and radiation, as well as corticosteroids, simultaneously with the ketogenic diet. It is remarkable that during this time, glucose values did not typically rise above $80\mathrm{mg/dL}$ . Comparatively, glucose values were particularly elevated at end-of-life care while on concomitant chemotherapy and corticosteroids in non-adhering patients.
在坚持饮食干预的6名患者中观察到独特特征(表 3)。患者1(P1)接受了放疗联合$75:\mathrm{mg}/\mathrm{m}^{2}$替莫唑胺治疗1个月,随后以$180:\mathrm{mg/m}^{2}$剂量维持治疗(每月5天),持续24个月后停药。总计接受同步放化疗$+\mathrm{KD}$治疗24个月,后续观察期(60个月)仅采用生酮饮食。其ECOG体能状态评分为0分(完全正常活动)。患者P2目前存活43个月,其中36个月接受生酮饮食治疗,ECOG评分为1分。患者P3中断生酮饮食后很快复发,初期接受化疗和可的松治疗时血糖未升高,化疗结束后重启生酮饮食,目前ECOG恢复至1分。6例患者均在接受生酮饮食期间同步接受放化疗及皮质类固醇治疗。值得注意的是,治疗期间血糖值通常未超过$80\mathrm{mg/dL}$。相比之下,未坚持饮食干预的患者在临终关怀期间接受联合化疗和皮质类固醇治疗时,血糖值显著升高。
5 Discussion
5 讨论
In our cohort, out of the 18 patients, 6 followed the diet for the predefined period of ${>}6$ months. The effects of the ketogenic diet observed in these six IDH-wild type GBM patients who adhered to the diet are promising, especially when compared to the disease progression in patients who were unable to maintain the diet, as well as to historical controls (1, 35–37). Two of them died after having lived 43 and 36 months, a period considerably longer than the average lifespan of patients with GBM (patient 4 and 6 respectively). The remaining 4 are still alive, with one completing 84 months of life (patient 1), while the other three remain alive at 43, 33 and 44 months (patients 2, 3, and 5 respectively). It should be noted that all adhering patients (with the exception of patient 1) continued intermittent chemotherapy. Therefore, the first question that arises is whether the ketogenic state contributed to the longer survival due to its effects on cancer metabolism, by potenti a ting chemotherapy, or both. We believe that the metabolic effects of the diet contributed to improved outcomes because the patients that did not receive it, or were not able to adhere to it, still receiving other standard of care treatments, exhibited shorter survival in our cohort.
在我们的队列中,18名患者中有6人坚持了预定义的 ${>}6$ 个月生酮饮食。这六名坚持饮食的IDH野生型胶质母细胞瘤(GBM)患者中观察到的效果令人鼓舞,尤其是与未能维持饮食的患者疾病进展以及历史对照数据相比 (1, 35–37)。其中两名患者分别存活43个月和36个月后离世(患者4和6),这一生存期显著长于GBM患者的平均生存期。其余4名患者目前仍存活,其中1人已生存84个月(患者1),另外三人分别存活43、33和44个月(患者2、3和5)。需注意的是,除患者1外,所有坚持饮食的患者均持续接受间歇性化疗。因此,首要问题是生酮状态通过影响癌症代谢、增强化疗效果,还是两者共同作用延长了生存期。我们认为饮食的代谢效应改善了预后,因为未接受或无法坚持该饮食但仍在接受其他标准治疗的患者,其生存期在本队列中更短。

Patient 6: (A) brain MRI on diagnosis (T2/FLAIR) (B) brain MRI on diagnosis (T1 with contrast) (C) 18-month follow up brain MRI (T1 with contrast) (D) 24-month follow-up brain MRI (T1 with contrast).
患者6:(A) 诊断时脑部MRI (T2/FLAIR) (B) 诊断时脑部MRI (T1增强) (C) 18个月随访脑部MRI (T1增强) (D) 24个月随访脑部MRI (T1增强)。

FIGURE 10 Study flow chart. pd, post diagnosis; ECOG, Eastern Cooperative Oncology Group.
图 10: 研究流程图。pd (post diagnosis), ECOG (Eastern Cooperative Oncology Group)。
TABLE 4 Patients who followed the diet beyond 6 months.
| Patient | DD | KD initiation | KD maintenance | Disease progression | GKI | Survival | Most recent ECOG Grade |
| P1 | 29/12/16 | 05/03/17 | 82 months | No evidence of disease progression | 1.09-2.78 | Still alive 84 months | 0 |
| P2 | 28/05/20 | 19/08/20 | 41 months | No evidence of disease progression | 0.83-2.1 | Still alive 43 months | 0 |
| P3 | 19/04/21 | 05/07/21 Stopped on January 22 Reinitiated May 22 | In total27months | 10/4/22 GBM relapse Cyberknife Reiniated KD | 1.46-3.7 | Still alive 33 months | 0 |
| P4 | 22/02/18 | 25/04/18 | 40 months | 10/20 GBM recurrence -surgical resection -15 cycles of radiation -Avastin | 1.26-2.36 | Died 8.9.2021 43 months | 5 |
| P5 | 24/04/20 | 27/04/20 | 40 months | Relapse | 1.17-2.93 | Still alive 44 months | 3 |
| P6 | 08/05/20 | 08/11/20 | 22 months in total | 8/2/22 cyberknife Avastin | 1.35-3.6 | Died 36 months | 5 |
P, Patients; P1-6, Patients whose numbers correspond to those in Table 1. DD, Diagnosis Date; GKI, glucose-ketone index; ECOG, Eastern Cooperative Oncology Group; ECOG Grade $0=$ Patient fully active, able to carry on all pre-disease performance without restriction, $1=$ Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or sedentary nature, e.g., light house work, office work, $2=$ Ambulatory and capable of all self-care but unable to carry out any work activities; up and about more than $50%$ of waking hours, $3=$ Capable of only limited self-care; confined to bed or chair.
表 4: 坚持饮食方案超过6个月的患者
| 患者 | 确诊日期(DD) | 生酮饮食启动(KD initiation) | 生酮饮食维持(KD maintenance) | 疾病进展(Disease progression) | 葡萄糖-酮体指数(GKI) | 生存期(Survival) | 最近ECOG评分(Most recent ECOG Grade) |
|---|---|---|---|---|---|---|---|
| P1 | 2016/12/29 | 2017/03/05 | 82个月 | 无疾病进展证据 | 1.09-2.78 | 存活84个月 | 0 |
| P2 | 2020/05/28 | 2020/08/19 | 41个月 | 无疾病进展证据 | 0.83-2.1 | 存活43个月 | 0 |
| P3 | 2021/04/19 | 2021/07/05(2022年1月停止 2022年5月重启) | 总计27个月 | 2022/4/10 GBM复发 接受射波刀治疗后重启生酮饮食 | 1.46-3.7 | 存活33个月 | 0 |
| P4 | 2018/02/22 | 2018/04/25 | 40个月 | 2020/10 GBM复发 -手术切除 -15次放疗 -阿瓦斯汀治疗 | 1.26-2.36 | 2021/9/8死亡(43个月) | 5 |
| P5 | 2020/04/24 | 2020/04/27 | 40个月 | 复发 | 1.17-2.93 | 存活44个月 | 3 |
| P6 | 2020/05/08 | 2020/11/08 | 总计22个月 | 2022/2/8接受射波刀和阿瓦斯汀治疗 | 1.35-3.6 | 死亡(36个月) | 5 |
P代表患者;P1-6编号与表1对应。DD:确诊日期;GKI:葡萄糖-酮体指数;ECOG:美国东部肿瘤协作组;ECOG评分标准:$0=$ 患者完全活跃,能无限制进行所有病前活动;$1=$ 体力活动受限但可行走,能从事轻量工作或久坐性质工作(如轻家务/办公室工作);$2=$ 可行走且生活自理,但不能工作;清醒时间超过$50%$处于活动状态;$3=$ 仅能有限自理;需卧床或坐轮椅。
TABLE 5 Survival of patients who did not follow the diet. Patients 7–18 are therefore the same patients as numbered in Table 1.
表 5: 未遵循饮食方案患者的生存情况。患者7-18与表1中的患者编号相同。
| 患者 | 性别 | 年龄 | 总生存期 |
|---|---|---|---|
| P7 | 男 | 60 | 12个月 |
| P8 | 男 | 69 | 6个月 |
| P9 | 男 | 53 | 14个月 |
| P10 | 女 | 57 | 14个月 |
| P11 | 女 | 36 | 25个月 |
| P12 | 女 | 44 | 29个月 |
| P13 | 女 | 34 | 存活36个月 |
| P14 | 女 | 59 | 17个月 |
| P15 | 男 | 51 | 18个月 |
| P16 | 女 | 75 | 12个月 |
| P17 | 女 | 59 | 19个月 |
| P18 | 男 | 71 | 11个月 |
When considering the patients as a whole, there was no significant difference in age between those who followed the diet and those who did not (average age of participants: $54.66\pm8.6$ , non-participants: $55.66\pm12.9$ ).
将患者作为整体考虑时,遵循饮食方案者与未遵循者在年龄上无显著差异(参与者平均年龄: $54.66\pm8.6$,非参与者: $55.66\pm12.9$)。
There was concern regarding the significant number of patients who did not adhere to the diet, despite it being recommended to all and thoroughly explained, including its principles and expected outcomes. An attempt was made to uncover the reasons why these patients ultimately did not follow the diet. One potential reason for non-adherence to the diet in certain cases was the strong desire of close relatives to avoid discussing the seriousness of the diagnosis and the unfavorable prognosis with the patients. This applied to three of our patients who had already undergone surgical resection, radiation, and chemotherapy. They felt reassured that they had done everything possible and saw no need to adhere to a demanding diet. Another reason was a lack of trust in the diet; four of our patients did not believe that, following conventional therapies, a simple diet could be beneficial, despite initially agreeing to follow it. Older patients, in particular, struggled to adjust their eating habits and discontinued the diet shortly after starting. Additionally, two patients stopped the diet due to the absence of a supportive environment, while another two discontinued it due to financial constraints, as they found the ketogenic diet to be relatively costly to implement.
尽管向所有患者详细解释了饮食原则及预期效果,但仍有大量患者未遵循饮食建议,这一现象引发了担忧。我们试图探究这些患者最终未坚持饮食方案的原因。在某些病例中,亲属强烈回避向患者透露诊断的严重性和不良预后,这成为依从性差的重要原因——三名已完成手术切除、放疗和化疗的患者因此认为已竭尽所能,无需再坚持严苛的饮食。另有四名患者对饮食疗法缺乏信任,尽管最初同意尝试,他们不相信传统治疗结束后简单饮食能带来益处。老年患者尤其难以改变饮食习惯,往往刚开始便放弃。此外,两名患者因缺乏支持环境而中止,另两名则因生酮饮食实施成本较高而受经济限制退出。
Another challenge encountered was the significant number of women who did not adhere to the diet. Out of the 8 women who participated, only one adhered to the diet, while the remaining 7 did not. While there are distinct differences in the path o physiology of the disease between men and women, none of these differences can adequately explain these findings. Sex differences in glioblastoma patients have been well documented, with evidence suggesting that women tend to respond better than men to conventional treatments for this disease (38–40). Could these differences influence the effect of the ketogenic diet in the patients of this study? The number of participants is small, and among the 6 patients, only one is a woman. Larger studies, separating men and women, will certainly be necessary. Regarding the non-participants, it is interesting to note that women appear to have a longer life expectancy than men. However, analyzing this data is beyond the scope of the current study. Furthermore, the relatively small sample size in the study prevents drawing definitive conclusions.
遇到的另一个挑战是大量女性患者未坚持饮食方案。在参与的8名女性中,仅1人遵守饮食规定,其余7人未遵守。虽然男女患者的疾病病理生理学存在明显差异,但这些差异都无法合理解释上述现象。胶质母细胞瘤患者的性别差异已有充分文献记载,证据表明女性对该疾病常规治疗的反应通常优于男性[38-40]。这种差异是否会影响生酮饮食对本研究患者的效果?本次参与者数量较少,6名患者中仅1名为女性。未来必然需要开展更大规模、区分性别的研究。值得注意的是,在未参与者中,女性似乎比男性具有更长的预期寿命。但分析这一数据超出了本研究范围。此外,相对较小的样本量也阻碍了得出明确结论。
It is difficult to ascertain whether a synergistic effect could be present given our study design and number of participants. Previous clinical experiences showed that the ketogenic diet may increase the effectiveness of radiation in pancreatic and lung cancer, but the long-term interactions between radiotherapy and metabolic targeting in GBM are unknown (41). As far as we know, there are no studies evaluating the synergy between the ketogenic diet and standalone chemotherapy in patients with GBM. Several experimental and clinical reports explored the combination of chemotherapy and ketogenic diets in other forms of cancer. For example, in a recent experimental study, Yang et al. (42) demonstrated that the ketogenic diet sensitizes murine pancreatic cancer tumors to cytotoxic chemotherapy. There is limited but encouraging clinical data regarding the co-administration of a ketogenic diet and chemotherapy in patients with neuroblastoma, as well as breast, pancreatic and gastric cancer (43–48).
鉴于我们的研究设计和参与者数量,很难确定是否存在协同效应。先前的临床经验表明,生酮饮食可能增强胰腺癌和肺癌放疗效果,但放疗与代谢靶向治疗在胶质母细胞瘤(GBM)中的长期相互作用尚不明确 (41) 。据我们所知,目前尚无研究评估生酮饮食与单纯化疗在GBM患者中的协同作用。若干实验和临床报告探讨了化疗与生酮饮食在其他癌症类型中的联合应用。例如,Yang等人在近期实验研究中 (42) 证实生酮饮食能增强细胞毒性化疗对小鼠胰腺癌肿瘤的敏感性。关于神经母细胞瘤、乳腺癌、胰腺癌和胃癌患者联合使用生酮饮食与化疗的临床数据虽然有限但结果积极 (43–48) 。
Each of our patients differed in chemotherapy schedules. We wish to highlight patient 1, presenting with an IDH wild-type GBM, which has lived 84 months so far with an ECOG score 0. He has maintained the ketogenic diet as the only treatment modality for the last 5 years without recurrence and without chemotherapy. The remaining three surviving patients experienced recurrence and underwent chemotherapy again. Interestingly, no metabolic dys regulation was observed during chemotherapy and cor tico steroid administration. More specifically, glucose levels did not exceed $80\mathrm{mg/dL}$ and satisfactory ketosis was maintained. It has been well established that patients undergoing cor tico steroid administration show increased levels of glycemia, lactate and insulin, with an unfavorable effect on tumor progression (49–55). The administration of ketogenic diets during chemotherapy and/or corticosteroids may benefit cancer patients through the control of metabolic dys regulation, beyond direct effects on cancer cells.
每位患者的化疗方案各不相同。我们特别要强调患者1,其IDH野生型胶质母细胞瘤(GBM)至今已存活84个月,ECOG评分为0分。过去5年,他仅依靠生酮饮食作为唯一治疗方式,未出现复发且未接受化疗。其余三名存活患者均经历复发并再次接受化疗。值得注意的是,在化疗和皮质类固醇(corticosteroid)治疗期间未观察到代谢失调现象。具体而言,血糖水平始终未超过$80\mathrm{mg/dL}$,且保持理想酮症状态。现有研究充分证实[49-55],接受皮质类固醇治疗的患者会出现血糖、乳酸和胰岛素水平升高,这对肿瘤进展产生不利影响。在化疗和/或皮质类固醇治疗期间采用生酮饮食,可能通过调控代谢紊乱(而非直接作用于癌细胞)使癌症患者获益。
Another noteworthy observation is that all patients with the longest survival were IDH mutant negative. IDH mutations have been associated with better prognosis in high-grade gliomas (IDH mutant grade 4 astrocytomas are no longer considered “true” GBM in the 2021 WHO classification). However, while long-term survivors have been reported in IDH “wild-type” GBM, the proportion of patients surviving over 5 years in unselected GBM populations is exceedingly small (56). It would therefore be expected that long-term survivors in our cohort would present IDH mutations, but this was not the case. Further studies will be needed to determine whether dietary KMT can benefit GBM patients regardless of IDH mutation status.
另一个值得注意的观察结果是,所有生存期最长的患者均为IDH突变阴性。在高级别胶质瘤中,IDH突变通常与较好预后相关(根据2021年WHO分类,IDH突变型4级星形细胞瘤不再被视为"真正"的GBM)。然而,虽然IDH"野生型"GBM中也有长期存活病例的报道,但在未经筛选的GBM患者群体中存活超过5年的比例极低[56]。因此,我们原本预期队列中的长期存活者会存在IDH突变,但实际情况并非如此。后续需要进一步研究来确定饮食KMT是否不论IDH突变状态都能使GBM患者获益。
None of the patients who followed the diet developed dys lipid emi a or reported major side effects. We suggest that the Mediterranean-type ketogenic diet may be suitable for at-risk patient populations such as cancer patients, offering more dietary flexibility than the classical 4:1 ketogenic diet used in epilepsy research (57).
遵循该饮食方案的患者均未出现血脂异常或报告严重副作用。我们认为地中海式生酮饮食可能适合癌症患者等高危人群,相比癫痫研究中使用的经典4:1生酮饮食 (57) 具有更高的膳食灵活性。
Tumor recurrence despite diet adherence can be explained by secondary metabolic dependencies of tumor cells (58–61). It is important to acknowledge that dietary strategies alone, such as ketogenic diets or fasting, cannot fully deplete glucose from the tumor micro environment. Dietary KMT intends to reduce pro-growth signaling, normalize the tumor micro environment, and increase substrate competition between cancer and non-tumoral cells, but p harm a co logical metabolic targeting was not employed in this study. Glut amino lysis is recognized as the second major energy pathway in cancer and cannot be targeted using dietary strategies alone. Given that glut amino lysis was not targeted in this study, we hypothesize that glutamine dependence may have contributed to incomplete responses. Interestingly, some researchers disagree about the action of fats as cancer cell growth inhibitors and believe the opposite. Article by Sperry et al. concludes that glioblastoma utilizes fatty acids and ketone bodies for growth allowing progression during KMT therapy (62). Similar conclusions are drawn by an article by Duman et al. (63) demonstrating that the availability of fatty acyl-CoA into mitochondria is driving b-oxidation and promotes tumor i genesis. But both of the above mentioned papers are having a different goal from KMT. Their goal is to maintain SLP, and target FAO. The goal with KMT is to target SLP, and maintain FAO/ OXPHOS. Consequently, proliferation rates will go down if fatty acid “utilization” is targeted. Fatty acids are used for biomass, when available (as per labeling), and partially “respired.”
尽管坚持饮食控制仍出现肿瘤复发,这可以用肿瘤细胞的次级代谢依赖性来解释 [58-61]。需要明确的是,仅靠生酮饮食或禁食等膳食策略无法完全清除肿瘤微环境中的葡萄糖。饮食性KMT旨在减少促生长信号、使肿瘤微环境正常化,并增强癌细胞与非肿瘤细胞间的底物竞争,但本研究未采用药理学代谢靶向干预。谷氨酰胺分解作为癌症的第二大能量代谢途径,无法仅通过饮食策略进行靶向。鉴于本研究未针对谷氨酰胺分解通路,我们推测谷氨酰胺依赖性可能是导致疗效不完全的原因。值得注意的是,部分研究者对脂肪抑制癌细胞生长的作用持相反观点。Sperry等人的论文指出,胶质母细胞瘤会利用脂肪酸和酮体促进生长,导致KMT治疗期间病情进展 [62]。Duman等 [63] 的研究也得出类似结论,证明脂肪酰基CoA进入线粒体可驱动β氧化并促进肿瘤发生。但这两项研究的目标与KMT不同:前者旨在维持底物水平磷酸化(SLP)并靶向脂肪酸氧化(FAO),而KMT的目标是靶向SLP并维持FAO/氧化磷酸化(OXPHOS)。因此,若靶向脂肪酸"利用"将降低增殖速率——根据标记实验,现有脂肪酸会被用于生物质合成,部分参与"呼吸"代谢。
Furthermore (64), radiation therapy may contribute to secondary metabolic reprogramming, increased tissue inflammation and heightened aggressiveness of the recurrent GBM cells, despite shortterm cytotoxic effects. Given the design of this study, with all patients undergoing conventional cycles of radiotherapy, it is not possible to discern whether surviving cancer cell populations may have displayed different metabolic responses if chemotherapy was administered as a standalone therapy.
此外 (64),放疗可能导致继发性代谢重编程、组织炎症加剧以及复发性胶质母细胞瘤细胞的侵袭性增强,尽管短期内具有细胞毒性作用。鉴于本研究的设计,所有患者均接受了常规放疗周期,因此无法确定若单独采用化疗,存活的癌细胞群体是否会表现出不同的代谢反应。
The encouraging results of our adhering participants highlight the importance of patient retention in ketogenic diet studies, with focus on pal at ability, reducing diet restrictive ness by leveraging modern food technologies (e.g., alternative recipes to common high-carbohydrate foods; non-caloric, non-insulin o geni c sweeteners), and avoiding participant drop-out by dedicated nutritional support.
我们坚持参与者的积极结果凸显了生酮饮食研究中患者保留的重要性,重点关注适口性、利用现代食品技术(例如常见高碳水化合物食品的替代配方;无热量、非胰岛素原性甜味剂)降低饮食限制性,并通过专门的营养支持避免参与者退出。
Patients with GBM experience reduced quality of life due to the disease itself, surgical resection and intensive che mo radio therapeutics regimens. As a consequence, it may be difficult to introduce overwhelming changes to their daily routines, food choices or lifestyle habits (65–67). It is therefore essential to describe the scientific rationale behind dietary KMT to both the patient and their caregivers to improve diet adherence, fostering patient autonomy.
GBM患者因疾病本身、手术切除和强化放化疗方案导致生活质量下降。因此,对他们的日常生活、饮食选择或生活习惯进行重大改变可能较为困难 [65-67]。因此,必须向患者及其照护者解释生酮代谢疗法 (KMT) 的科学依据,以提高饮食依从性,增强患者的自主性。
Another challenge for diet implementation is finding compatibility with conventional treatments and traditional dietary advice for cancer patients. To make the application of ketogenic diets more widely accessible, it is fundamental for both the patient and their treating oncologist to discuss the available experimental and clinical data on a case-by-case basis. A review published by Valerio et al. (68) included all prospective, retrospective, and randomized clinical studies, as well as case reports on the use of KD as an adjunctive therapy for primary brain tumors, including recurrent and newly diagnosed GBM. These studies exhibited significant heterogeneity in their design, tumor type, diet implementation and duration, number of participants, patient demographics, and outcome measures. Consequently, comparing the results of these studies with one another—and with our own study, which focused exclusively on patients with newly diagnosed GBM— presents substantial challenges. Overall, KD was generally welltolerated across the studies, although adherence proved difficult due to the diet’s restrictive nature. Survival outcomes varied, with some studies indicating potential benefits in specific subgroups, such as younger patients or those with favorable genetic markers like IDH1 mutations. Median overall survival (OS) across the studies ranged from 8 to 60 months, with the majority reporting improved overall survival compared to the known median survival time associated with standard therapy for GBM. However, small sample sizes and methodological differences limit the broader applicability of these results. Undoubtedly, further research involving larger, more homogeneous patient cohorts and standardized ketogenic diet protocols is needed to reach more definitive conclusions. To summarize, an in-depth evaluation of the scientific literature, which shows beneficial effects on survival, quality of life and self- efficacy, is essential prior to starting this intervention (10, 13, 16, 24, 69–73).
实施生酮饮食的另一项挑战在于如何与传统癌症治疗方法和常规饮食建议相兼容。为使生酮疗法更广泛适用,患者与肿瘤医生必须根据具体病例讨论现有实验及临床数据。Valerio等学者发表的综述[68]涵盖了所有前瞻性、回顾性、随机临床研究以及生酮饮食辅助治疗原发性脑肿瘤(包括新诊断和复发性胶质母细胞瘤)的病例报告。这些研究在设计方案、肿瘤类型、饮食执行周期、参与者数量、患者人口统计学特征及疗效评估指标等方面存在显著异质性,导致研究结果难以相互比较——也难与本研究(仅针对新诊断胶质母细胞瘤患者)直接对照。总体而言,各研究中生酮饮食耐受性良好,但限制性特征导致依从性较差。生存结局存在差异:部分研究显示特定亚组(如年轻患者或携带IDH1突变等有利遗传标志物者)可能获益。各研究的中位总生存期(OS)介于8至60个月,多数报告显示较标准疗法已知中位生存期有所延长。然而样本量不足和方法学差异限制了结果的普适性。显然,需要更大规模、更同质化的患者队列和标准化生酮方案来获得明确结论。综上,启动该干预措施前,必须系统评估显示其对生存率、生活质量和自我效能存在积极影响的科学文献(10, 13, 16, 24, 69–73)。
Lastly, interventional dietary studies require special attention to methodology and planning to ensure the patient is well-informed and eventually able to make decisions regarding food choices without constant guidance. This is self-evident if we consider that the “diet intervention” is expected to last several years. Accordingly, it will be important to integrate dietary KMT as part of the standard of care, rather than relying on patient autonomy to external ize it as a complementary treatment modality. It is important to mention that the suitability of the ketogenic diet should be evaluated by a dietitian, neurologist, oncologist and/or neurosurgeon specializing in ketogenic diets. The number of healthcare professionals familiar with nutritional ketosis and its practical applications is growing due to renewed interest in metabolic interventions for chronic diseases (74). This will facilitate adherence in future clinical studies, building from individual clinical experiences and moving into larger clinical trials.
最后,饮食干预研究需要特别关注方法和规划,以确保患者充分知情并最终能够在没有持续指导的情况下自主决定食物选择。如果我们考虑到"饮食干预"预计将持续数年,这一点就不言而喻了。因此,将生酮代谢疗法(KMT)纳入标准治疗方案至关重要,而不是依赖患者自主将其外部化为补充治疗方式。需要特别指出的是,生酮饮食的适用性应由专门研究生酮饮食的营养师、神经科医生、肿瘤科医生和/或神经外科医生进行评估。由于对慢性病代谢干预重新产生兴趣[74],熟悉营养性酮症及其实际应用的医疗专业人员数量正在增加。这将有助于未来临床研究的依从性,从个体临床经验出发,逐步推进到更大规模的临床试验。
6 Conclusion
6 结论
In our study, patients who followed a well-designed ketogenic diet had longer survival compared to patients who did not follow it. Although the number of patients is small, the results are encouraging and motivate us to plan studies with a larger number of patients, where we will examine the effects of the diet separately in women and men. Furthermore, when the ketogenic diet was applied alongside chemotherapy and corticosteroids, no dysfunction in glucose metabolism was observed. This is very important and perhaps the deepest message of our work, as we know that cancer cells exhibit altered and increased glucose uptake and increased glycolysis, which was first recognized by Otto Warburg 70 years ago (7, 8). It is also well known that both chemotherapy and steroids increase glycolysis (75, 76). Therefore, on one hand, they have a beneficial effect, but on the other hand, they promote the growth of cancer cells by increasing glycolysis (64, 77). And this is precisely where the important contribution of the ketogenic diet lies, which, as shown by our results, helps to prevent the metabolic dys regulation resulting from conventional treatment for glioblastoma (78–81). The ketogenic diet, however, could have other contributions to the treatment of these patients. Brain tumors rely energetically on glycolysis, unlike healthy neurons/glial cells, which can alternatively consume ketone bodies. Thus, ketone bodies have a toxic effect on cancer cells while leaving healthy cells unaffected. So, it seems that the mechanisms of diet work at multiple levels, thus helping to prolong the survival of these patients. The number of patients in our study is small, but it gives us an important incentive to perform larger studies with a larger number of patients, in the hope of providing another weapon in the treatment of this incurable brain tumor.
在我们的研究中,遵循精心设计的生酮饮食的患者比未遵循者生存期更长。尽管患者数量较少,但结果令人鼓舞,促使我们计划开展更大规模的研究,分别考察该饮食对女性和男性的影响。此外,当生酮饮食与化疗和皮质类固醇联用时,未观察到葡萄糖代谢异常。这一点至关重要,或许是我们工作中最深层的启示——正如70年前Otto Warburg首次发现的那样[7,8],癌细胞会表现出异常增强的葡萄糖摄取和糖酵解作用。而化疗和类固醇都会促进糖酵解[75,76],这种双重性既产生治疗效果,又通过增强糖酵解助长癌细胞生长[64,77]。这正是生酮饮食的重要价值所在:我们的结果表明,它能防止胶质母细胞瘤常规治疗导致的代谢失调[78-81]。生酮饮食还可能通过其他机制发挥作用。与能利用酮体的健康神经元/胶质细胞不同,脑肿瘤的能量供应高度依赖糖酵解,因此酮体对癌细胞具有选择性毒性。这种多层次的协同机制有望延长患者生存期。虽然本研究样本量有限,但为后续大规模研究提供了重要依据,或将为这种难治性脑肿瘤的治疗增添新武器。
Data availability statement
数据可用性声明
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
支持本文结论的原始数据将由作者在无不当保留的情况下提供。
Ethics statement
伦理声明
The studies involving humans were approved by the Aristotle University of Thessaloniki Ethics Committee (PN 1232/16). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual (s) for the publication of any potentially identifiable images or data included in this article.
涉及人类参与的研究已获塞萨洛尼基亚里士多德大学伦理委员会批准(PN 1232/16)。研究过程严格遵守当地法律法规及机构要求。所有参与者均签署书面知情同意书自愿参加本研究,并就本文中可能包含的可识别图像或数据获取了个人书面授权发布许可。
Author contributions
作者贡献
AK: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Data curation, Formal analysis, Investigation, Validation, Visualization. AE: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Project administration, Supervision. IK: Writing – review & editing, Data curation, Investigation. IB: Conceptualization, Writing – original draft, Writing – review & editing, Investigation, Validation. NF: Writing – review & editing. BZ: Writing – review & editing. AC: Writing – original draft, Writing – review & editing, Data curation. VN: Data curation, Writing – original draft, Writing – review & editing. TZ: Data curation, Writing – review & editing. TD: Writing – review & editing. TS: Writing – original draft, Writing – review & editing. MS: Conceptualization, Project administration, Supervision, Writing – original draft, Writing – review & editing.
AK: 概念化、方法论、撰写初稿、评审与编辑、数据管理、形式分析、调查、验证、可视化。
AE: 概念化、方法论、撰写初稿、评审与编辑、项目管理、监督。
IK: 评审与编辑、数据管理、调查。
IB: 概念化、撰写初稿、评审与编辑、调查、验证。
NF: 评审与编辑。
BZ: 评审与编辑。
AC: 撰写初稿、评审与编辑、数据管理。
VN: 数据管理、撰写初稿、评审与编辑。
TZ: 数据管理、评审与编辑。
TD: 评审与编辑。
TS: 撰写初稿、评审与编辑。
MS: 概念化、项目管理、监督、撰写初稿、评审与编辑。
Funding
资金
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
作者声明未就本文的研究、撰写及/或发表获得任何资金支持。
Acknowledgments
致谢
The authors would like to thank Panayiotis Sel via rid is, Emeritus Professor of Neurosurgery, Aristotle University of Thessaloniki and Hamalidou Eleni Panagiota, Oncologist, AHEPA University Hospital for critically reviewing the manuscript and for their valuable contribution to this research.
作者感谢塞萨洛尼基亚里士多德大学神经外科名誉教授Panayiotis Sel via rid is和AHEPA大学医院肿瘤学家Hamalidou Eleni Panagiota对稿件进行严格审阅,并为本研究作出的宝贵贡献。
Conflict of interest
利益冲突
Author VN and TZ were employed by company Is to die rev ni tiki S.A. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
作者VN和TZ受雇于公司Is to die rev ni tiki S.A.。其余作者声明,该研究是在没有任何可能被解释为潜在利益冲突的商业或财务关系的情况下进行的。
Publisher’s note
出版商说明
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
本文表达的所有主张仅为作者个人观点,并不必然代表其所属机构、出版商、编辑及审稿人的立场。对于文中可能提及的任何产品或制造商声明,出版商不作任何担保或认可。
- Evangelou E, ilioti MG, Vassilakou D, Goutsaridu Seyfried T Restrit ketogenic diet therapy for primary lung Cancer with metastasis to the brain: a case report. Cureus. (2022) 14:e27603. doi: 10.7759/cureus.27603 25. Lussier DM, Woolf EC, Johnson JL, Brooks KS, Blattman JN, Scheck AC. Enhanced immunity in a mouse model of malignant glioma is mediated by a therapeutic ketogenic diet. BMC Cancer. (2016) 16:310. doi: 10.1186/s12885-016-2337-7 26.Liang J, LX, Lu C, YX, Chen X,Fu J et al. Prognostic factors of patients ith gliomas — an analysis on 335 patients with glioblastoma and other forms of gliomas. BMC Cancer. (2020) 20:35. doi: 10.1186/s12885-019-6511-6 27.Kartik R, LGR,Lee C, Tang PY, Grace K,Chua LMK, et al. Clinical prognostc factors of survival in glioblastoma multiforme (2593). Neurology. (2020) 94:2593. doi: 10.1212/WNL.94.15_supplement.2593 28. van der Louw EJTM Olieman J, van den Bemt PMA, Bromberg JEC, Oomen-de Hoop E, Neuteboom RF, et al. Ketogenic diet treatment as adjuvant to standard treatment of glioblastoma multiforme: a feasibility and safety study. Ther Adv Med Oncol. (2019) 11:1758835919853958. doi: 10.1177/1758835919853958 29. Kang HC, Chung DE, Kim DW, Kim HD. Early- and late-onset complications of the ketogenic diet for intractable epilepsy. Epilepsia. (2004) 45:1116–23. doi: 10.1111/j.0013-9580.2004.10004.x 30. Mohammadi E, Moghaddam SS, Azad najaf a bad S, Maroufi SE, Rashidi MM, Naderian M, et al. Epidemiology of brain and other central nervous system cancers in the North Africa and Middle East region: a systematic analysis of the global burden of disease study 1990-2019. World Neurosurg X. (2023) 171:e796–819. doi: 10.1016/j. wneu.2022.12.112 31. DyLE, Ong E Espiritu AI Spears J Omar AT 2nd. Survival times of patients with glioblastoma in low- and middle-income countries: a systematic review and metaanalysis. Neurosurg Rev. (2022) 45:3393–403. doi: 10.1007/s10143-022-01844-x 32. Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET, et al. Toxicity and response criteria of the eastern cooperative oncology group. Am J Clin Oncol. (1982) 5:649–56. doi: 10.1097/00000421-198212000-00014 33.Evangeliu A, Spiloti M,Douloglou V Kala d poul ou P, liasA,Skarpalzou , et al. Branched chain amino acids as adjunctive therapy to ketogenic diet in epilepsy: pilot study and hypothesis. J Child Neurol. (2009) 24:1268–72. doi: 10.1177/0883073809336295 34.Evangelu A,Vahniklis I,MihaiidouH Spilt i Mara leu Makaronas N, et al. Application of a ketogenic diet in children with autistic behavior: pilot study. J Child Neurol. (2003) 18:113–8. doi: 10.1177/08830738030180020501 35.Huan nt fn ma antz lm h th on primary glioblastoma patient survival. BMC Neurol. (2021) 21:424. doi: 10.1186/ s12883-021-02461-9 36.Kawauchi D, Ono M, Honda-Kitahara M, Miyakita Y, Takahashi M, Yanagisawa S, et al. Clinical characteristics and prognosis of glioblastoma patients with infra ten to rial recurrence. BMC Neurol. (2023) 23:9. doi: 10.1186/s12883-022-03047-9 37.Chen L, Ma J, Zou Z, Liu H, Liu C, Gong S, et al. Clinical characteristics and prognosis of patients with glioblastoma: a review of survival analysis of 1674 patients based on SEER database. Medicine. (2022) 101:e32042. doi: 10.1097/ MD.0000000000032042 38.Colopi A,Fuda S, Santi S, Onorato A,Cesarini V, Salvati M, et al. mpact of ag and gender on glioblastoma onset, progression, and management. Mech Ageing Dev. (2023) 211:111801. doi: 10.1016/j.mad.2023.111801 39.CaraAanD aGCazaH differences in glioblastoma. Cells. (2021) 10:1783. doi: 10.3390/cells10071783 40. Jang B, Yoon D, Lee JY, Kim J, Hong J, Koo H, et al. Integrative multi-omics characterization reveals sex differences in glioblastoma. Biol Sex Differ. (2024) 15:23. doi: 10.1186/s13293-024-00601-7 4.Zan diet while receiving radiation and chemotherapy for locally advanced lung cancer and pancreatic cancer: the university of Iowa experience of two phase 1 clinical trials. Radiat Res. (2017) 187:743–54. doi: 10.1667/RR14668.1 42.Yang L, Tela T, Ng S, Nofal M, Wang L, Lan T, et al. Ketogenic diet and chemotherapy combine to disrupt pancreatic cancer metabolism and growth. J Med. (2022) 3:119–36. doi: 10.1016/j.medj.2021.12.008 43.A miz aGa hG VLt hd M, et al. A ketogenic diet supplemented with medium-chain triglycerides enhances the anti-tumor and anti-angiogenic efficacy of chemotherapy on neuroblastoma xenografts in a CD1-nu mouse model. Oncotarget. (2017) 8:64728–44. doi: 10.18632/ oncotarget.20041 44. Kirkham AA, King K, Joy AA, Pelletier AB, Mackey , Young K, et al. Ratiol and design of the diet restriction and exercise-induced adaptations in metastatic breast cancer (DREAM) study: a 2-arm, parallel-group, phase II, randomized control trial of a short-term, calorie-restricted, and ketogenic diet plus exercise during intravenous chemotherapy versus usual care. BMC Cancer. (2021) 21:1093. doi: 10.1186/ s12885-021-08808-2
- Evangelou E, Ilioti MG, Vassilakou D, Goutsaridou Seyfried T. 限制性生酮饮食治疗原发性肺癌脑转移病例报告。Cureus. (2022) 14:e27603. doi: 10.7759/cureus.27603
- Lussier DM, Woolf EC, Johnson JL, Brooks KS, Blattman JN, Scheck AC. 生酮饮食增强恶性胶质瘤小鼠模型的免疫反应。BMC Cancer. (2016) 16:310. doi: 10.1186/s12885-016-2337-7
- Liang J, LX, Lu C, YX, Chen X, Fu J 等. 胶质瘤患者预后因素分析——基于335例胶质母细胞瘤及其他胶质瘤的研究。BMC Cancer. (2020) 20:35. doi: 10.1186/s12885-019-6511-6
- Kartik R, LGR, Lee C, Tang PY, Grace K, Chua LMK 等. 多形性胶质母细胞瘤生存期的临床预后因素(2593)。Neurology. (2020) 94:2593. doi: 10.1212/WNL.94.15_supplement.2593
- van der Louw EJTM, Olieman J, van den Bemt PMA, Bromberg JEC, Oomen-de Hoop E, Neuteboom RF 等. 生酮饮食作为多形性胶质母细胞瘤标准治疗辅助方案的可行性与安全性研究。Ther Adv Med Oncol. (2019) 11:1758835919853958. doi: 10.1177/1758835919853958
- Kang HC, Chung DE, Kim DW, Kim HD. 难治性癫痫生酮饮食治疗的早晚期并发症。Epilepsia. (2004) 45:1116–23. doi: 10.1111/j.0013-9580.2004.10004.x
- Mohammadi E, Moghaddam SS, Azad Najafabad S, Maroufi SE, Rashidi MM, Naderian M 等. 北非和中东地区脑及其他中枢神经系统肿瘤流行病学:1990-2019年全球疾病负担系统分析。World Neurosurg X. (2023) 171:e796–819. doi: 10.1016/j.wneu.2022.12.112
- Dy LE, Ong E, Espiritu AI, Spears J, Omar AT 2nd. 中低收入国家胶质母细胞瘤患者生存时间的系统评价与荟萃分析。Neurosurg Rev. (2022) 45:3393–403. doi: 10.1007/s10143-022-01844-x
- Oken MM, Creech RH, Tormey DC, Horton J, Davis TE, McFadden ET 等. 东部肿瘤协作组毒性及疗效评价标准。Am J Clin Oncol. (1982) 5:649–56. doi: 10.1097/00000421-198212000-00014
- Evangeliu A, Spiloti M, Douloglou V, Kaladopoulou P, Ilias A, Skarafzou 等. 支链氨基酸作为癫痫生酮饮食辅助治疗的初步研究及假说。J Child Neurol. (2009) 24:1268–72. doi: 10.1177/0883073809336295
- Evangelu A, Vahniklis I, Mihaiidou H, Spiliti M, Araleu M, Makaronas N 等. 生酮饮食在自闭症行为儿童中的应用:初步研究。J Child Neurol. (2003) 18:113–8. doi: 10.1177/08830738030180020501
- Huant fn ma antz lm h th on 原发性胶质母细胞瘤患者生存分析。BMC Neurol. (2021) 21:424. doi: 10.1186/s12883-021-02461-9
- Kawauchi D, Ono M, Honda-Kitahara M, Miyakita Y, Takahashi M, Yanagisawa S 等. 幕下复发胶质母细胞瘤患者的临床特征及预后。BMC Neurol. (2023) 23:9. doi: 10.1186/s12883-022-03047-9
- Chen L, Ma J, Zou Z, Liu H, Liu C, Gong S 等. 基于SEER数据库1674例患者的胶质母细胞瘤临床特征及生存分析。Medicine. (2022) 101:e32042. doi: 10.1097/MD.0000000000032042
- Colopi A, Fuda S, Santi S, Onorato A, Cesarini V, Salvati M 等. 年龄与性别对胶质母细胞瘤发病、进展及治疗的影响。Mech Ageing Dev. (2023) 211:111801. doi: 10.1016/j.mad.2023.111801
- CaraAanD aGCazaH 胶质母细胞瘤的性别差异。Cells. (2021) 10:1783. doi: 10.3390/cells10071783
- Jang B, Yoon D, Lee JY, Kim J, Hong J, Koo H 等. 多组学整合分析揭示胶质母细胞瘤性别差异。Biol Sex Differ. (2024) 15:23. doi: 10.1186/s13293-024-00601-7
- Zan 局部晚期肺癌与胰腺癌放化疗期间生酮饮食:爱荷华大学两项I期临床试验经验。Radiat Res. (2017) 187:743–54. doi: 10.1667/RR14668.1
- Yang L, Tela T, Ng S, Nofal M, Wang L, Lan T 等. 生酮饮食联合化疗破坏胰腺癌代谢与生长。J Med. (2022) 3:119–36. doi: 10.1016/j.medj.2021.12.008
- A miz aGa hG VLt hd M 等. 中链甘油三酯强化生酮饮食增强神经母细胞瘤CD1-nu小鼠模型中化疗抗肿瘤及抗血管生成效果。Oncotarget. (2017) 8:64728–44. doi: 10.18632/oncotarget.20041
- Kirkham AA, King K, Joy AA, Pelletier AB, Mackey, Young K 等. DREAM研究方案设计:静脉化疗期间短期限热量生酮饮食联合运动对比常规治疗的II期随机对照试验。BMC Cancer. (2021) 21:1093. doi: 10.1186/s12885-021-08808-2
- Duman C, Yaqubi K, Hoffmann A, Acikgoz AA, Korshunov A, Bendszus M, et al. Acyl-CoA-binding protein drives glioblastoma tumor i genesis by sustaining fatty acid oxidation. Cell Metab. (2019) 30:274–89. doi: 10.1016/j.cmet.2019.04.004 64. Seyfried TN, Arismendi-Morillo G, Zuccoli G, Lee DC, Duraj T, Elsakka AM, et al. Metabolic management of micro environment acidity in glioblastoma. Front Oncol. (2022) 12:968351. doi: 10.3389/fonc.2022.968351 65. Caponnetto P, Schiliro G, Maglia M, Prez za vento GC, Baeken C, Health QMC, et al. Psychological and neuro psychological clinical impact in brain cancer patients and evidence-based psychological intervention: a systematic review of the literature. Health Psychol Res. (2024) 12:91408. doi: 10.52965/001c.91408 66. Seddighi A, Seddighi AS, Nikouei A, Ashraf F, Nohesara S. Psychological aspects in brain tumor patients: a prospective study. Hell J Nucl Med. (2015) 18:101389 67. Johnson DR. A focus on psychological needs of brain tumor patients and leveraging epidemiology. Neurooncol Pract. (2020) 7:463–4. doi: 10.1093/nop/npaa053 68. Valerio J, Borro M, Proietti E, Pisciotta L, Olarinde IO, Fernandez Gomez M, et al. Systematic review and clinical insights: the role of the ketogenic diet in managing glioblastoma in Cancer neuroscience. J Pers Med. (2024) 14:929. doi: 10.3390/j pm 14090929 69. Elsakka AMA, Bary MA, Abdelzaher E, Elnaggar M, Kalamian M, Mukherjee P et al. Management of GBM in a patient treated with. Ketogenic metabolic therapy and modified standard of care: a 24-month follow-up. Front Nutr. (2018) 5:20. doi: 10.3389/ fnut.2018.00020 70. Chino poul os C, Seyfried TN. Mitochondrial substrate-level phosphor yl ation as energy source for glioblastoma: review and hypothesis. ASN Neuro. (2018) 10:175909141881826. doi: 10.1177/1759091418818261 71. Schwartz L, Seyfried T,Alfarouk KO,Da Veiga MJ, Fais S. Out of Warburg eft an effective cancer treatment targeting the tumor specific metabolism and dys regulated pH. Semin Cancer Biol. (2017) 43:134–8. doi: 10.1016/j.semcancer.2017.01.005 72.Seyfrd,re RPf fMD Ago st nD M ker Metlicth a new paradigm for managing malignant brain cancer. Cancer Lett. (2015) 356:289–300. doi: 10.1016/j.canlet.2014.07.015 73. Pof AM, Ari C, Arnold P, Seyfried TN, D'Agostino DP Ketone supplement ation decreases tumor cell viability and prolongs survival of mice with metastatic cancer. Int J Cancer. (2014) 135:1711–20. doi: 10.1002/ijc.28809 74. Ludwig DS. The ketogenic diet: evidence for optimism but high-quality research needed. J Nutr. (2020) 150:1354–9. doi: 10.1093/jn/nxz308 75. Sonoda A, Yoshida N, Shiraishi S, Horinouchi T, Tokunaga R, Harada K, et al. Total lesion glycolysis ratio in positron emission tomography/computed tomography images during Neo ad juv ant chemotherapy can predict pathological tumor regression grade and prognosis in patients with locally advanced squamous cell carcinoma of the esophagus. Ann Surg Oncol. (2021) 28:167–74. doi: 10.1245/s10434-020-08738-6 76. Leighton B, Challis RA, Lozeman FJ, Newsholme EA. Effects of dex amet has one treatment on insulin-stimulated rates of glycolysis and glycogen synthesis in isolated incubated skeletal muscles of the rat. Biochem J. (1987) 246:551–4. doi: 10.1042/ bj2460551 77. Seyfried TN, Arismendi-Morillo G, Mukherjee P, Chino poul os C. On the origin of ATP synthesis in Cancer. iScience. (2020) 23:101761. doi: 10.1016/j.isci.2020.101761 78.Zhang Y, Tan H JaL,He J HaoPLi T, et al. Association of prperative gluose concentration with mortality in patients undergoing craniotomy for brain tumor. JNeurosurg. (2022) 138:1254–62. doi: 10.3171/2022.9.JNS221251 79. Flavahan WA, Wu Q, Hitomi M, Rahim N, Kim Y, Sloan AE, et al. Brain tumor initiating cells adapt to restricted nutrition through preferential glucose uptake. Nat Neurosci. (2013) 16:1373–82. doi: 10.1038/nn.3510 80. Yu J, Cao X, Zhou R, Chen Q, Wang Y. Abnormal brain glucose metabolism patterns in patients with advanced non-small-cell lung cancer after chemotherapy: a retrospective PET study. Brain Res Bull. (2023) 202:110751. doi: 10.1016/j. brain res bull.2023.110751 81. Schroyen G, Schramm G, Van Weehaeghe D, Leenaerts N, Vande Casteele T, Blommaert J, et al. Cerebral glucose changes after chemotherapy and their relation to long-term cognitive complaints and fatigue. Front Oncol. (2022) 12:1021615. doi: 10.3389/fonc.2022.1021615
- Duman C, Yaqubi K, Hoffmann A, Acikgoz AA, Korshunov A, Bendszus M, 等. 酰基辅酶A结合蛋白通过维持脂肪酸氧化驱动胶质母细胞瘤发生. 细胞代谢 (Cell Metab). (2019) 30:274–89. doi: 10.1016/j.cmet.2019.04.004
- Seyfried TN, Arismendi-Morillo G, Zuccoli G, Lee DC, Duraj T, Elsakka AM, 等. 胶质母细胞瘤微环境酸度的代谢调控. 肿瘤学前沿 (Front Oncol). (2022) 12:968351. doi: 10.3389/fonc.2022.968351
- Caponnetto P, Schiliro G, Maglia M, Prezzavento GC, Baeken C, Health QMC, 等. 脑癌患者心理与神经心理临床影响及循证心理干预:文献系统综述. 健康心理学研究 (Health Psychol Res). (2024) 12:91408. doi: 10.52965/001c.91408
- Seddighi A, Seddighi AS, Nikouei A, Ashraf F, Nohesara S. 脑肿瘤患者心理层面:前瞻性研究. 希腊核医学杂志 (Hell J Nucl Med). (2015) 18:101389
- Johnson DR. 聚焦脑肿瘤患者心理需求与流行病学应用. 神经肿瘤实践 (Neurooncol Pract). (2020) 7:463–4. doi: 10.1093/nop/npaa053
- Valerio J, Borro M, Proietti E, Pisciotta L, Olarinde IO, Fernandez Gomez M, 等. 系统综述与临床洞见:生酮饮食在癌症神经科学中管理胶质母细胞瘤的作用. 个性化医学杂志 (J Pers Med). (2024) 14:929. doi: 10.3390/jpm14090929
- Elsakka AMA, Bary MA, Abdelzaher E, Elnaggar M, Kalamian M, Mukherjee P 等. 采用生酮代谢疗法与改良标准护理治疗GBM患者的24个月随访管理. 营养前沿 (Front Nutr). (2018) 5:20. doi: 10.3389/fnut.2018.00020
- Chinopoulos C, Seyfried TN. 线粒体底物水平磷酸化作为胶质母细胞瘤能量来源:综述与假说. ASN神经科学 (ASN Neuro). (2018) 10:175909141881826. doi: 10.1177/1759091418818261
- Schwartz L, Seyfried T, Alfarouk KO, Da Veiga MJ, Fais S. 超越Warburg效应:靶向肿瘤特异性代谢与pH失调的有效癌症治疗. 癌症生物学研讨会 (Semin Cancer Biol). (2017) 43:134–8. doi: 10.1016/j.semcancer.2017.01.005
- Seyfried TN, Poff AM, Arismendi-Morillo G, Mukherjee P, Chinopoulos C. 代谢疗法:恶性脑癌管理新范式. 癌症快报 (Cancer Lett). (2015) 356:289–300. doi: 10.1016/j.canlet.2014.07.015
- Poff AM, Ari C, Arnold P, Seyfried TN, D'Agostino DP. 酮体补充降低肿瘤细胞活力并延长转移性癌症小鼠生存期. 国际癌症杂志 (Int J Cancer). (2014) 135:1711–20. doi: 10.1002/ijc.28809
- Ludwig DS. 生酮饮食:证据支持乐观但需高质量研究. 营养学杂志 (J Nutr). (2020) 150:1354–9. doi: 10.1093/jn/nxz308
- Sonoda A, Yoshida N, Shiraishi S, Horinouchi T, Tokunaga R, Harada K, 等. 新辅助化疗期间PET/CT图像中总病变糖酵解比率可预测局部晚期食管鳞癌患者病理肿瘤消退分级及预后. 外科肿瘤学年鉴 (Ann Surg Oncol). (2021) 28:167–74. doi: 10.1245/s10434-020-08738-6
- Leighton B, Challis RA, Lozeman FJ, Newsholme EA. 地塞米松处理对大鼠离体骨骼肌胰岛素刺激糖酵解与糖原合成速率的影响. 生物化学杂志 (Biochem J). (1987) 246:551–4. doi: 10.1042/bj2460551
- Seyfried TN, Arismendi-Morillo G, Mukherjee P, Chinopoulos C. 癌症中ATP合成起源探讨. iScience. (2020) 23:101761. doi: 10.1016/j.isci.2020.101761
- Zhang Y, Tan H, Jia L, He J, Hao P, Li T, 等. 脑肿瘤开颅手术患者术前血糖浓度与死亡率关联研究. 神经外科杂志 (J Neurosurg). (2022) 138:1254–62. doi: 10.3171/2022.9.JNS221251
- Flavahan WA, Wu Q, Hitomi M, Rahim N, Kim Y, Sloan AE, 等. 脑肿瘤起始细胞通过优先摄取葡萄糖适应营养限制. 自然神经科学 (Nat Neurosci). (2013) 16:1373–82. doi: 10.1038/nn.3510
- Yu J, Cao X, Zhou R, Chen Q, Wang Y. 晚期非小细胞肺癌化疗后患者脑葡萄糖代谢异常模式:回顾性PET研究. 脑研究通报 (Brain Res Bull). (2023) 202:110751. doi: 10.1016/j.brainresbull.2023.110751
- Schroyen G, Schramm G, Van Weehaeghe D, Leenaerts N, Vande Casteele T, Blommaert J, 等. 化疗后脑葡萄糖变化及其与长期认知障碍和疲劳的关系. 肿瘤学前沿 (Front Oncol). (2022) 12:1021615. doi: 10.3389/fonc.2022.1021615